
Alex writes:
Have you seen this?
From U.S. News and World Report: Over 150 Medical Experts Urge Trump, Congress and States to Shut U.S. Down Again Amid Virus Surge https://www.usnews.com/news/health-news/articles/2020-07-24/over-150-medical-experts-urge-trump-congress-and-states-to-shut-us-down-again-amid-coronavirus-surge
The letter: https://uspirg.org/resources/usp/shut-it-down-start-over-do-it-right
What do you folks at TWIV think about this? You’ve covered some letters people have written to Congress, etc but I don’t know if you’ve weighed in on this yet.
Thanks so much for your podcast, it’s been comforting to get factual information from your crew on this topic that is so important but not something I knew much about going into this crisis.
Alec
Denver, CO
Doug writes:
Just in case you did not see this USA Today coverage — with reference to TWIV :
Whether you’re infectious or not depends on how much virus your body is producing, Sikes said.
As someone is falling ill, the virus reproduces incredibly quickly, so they wouldn’t stay at low levels for more than a few hours, Mina said on a recent This Week in Virology podcast. Odds are slim the person would test themselves in that exact window and miss a burgeoning infection.
Doug
Dayton, Ohio
Rob writes:
Dear likeminded pedants,
I’m a retired Internet Architect. Its 20c and breezy here in Berkshire, England. I have a son who is a research immunologist at the NIH (Tcell receptors, NK cells etc.) A while back he said I should listen to something called TWIV with Jon Yewdell as there were some very clear descriptions of how parts of the immune system work, which I would probably understand, and my son and I might then be able to have more than a 3 word conversation about his research. That’s work in progress; but I did become fascinated by virology and since then I have been a regular LISTENER to TWIV, I LISTEN in the car, when I’m cooking, when I’m cutting the grass, but almost never have a screen in front of me at the time, so I would politely ask that you maintain the verbal descriptions of everything you cover in your podcasts and don’t start to rely on sharing images on Zoom, which recently, you seem to be doing more of. Being retired I just do not have the time to sit down and watch several hours of TWIV a week, and I would hate to miss it, a beacon of light in the murk of misinformation.
Keep up the great science and scientific method.
Rob
PS As a newbie could you explain how you can have a single R0 for a virus independent of the society in which the virus exists. Surely the value is different for a respiratory virus (say) in a society where people greet each other by kissing on both cheeks compared to one in which people bow a metre or so apart. Or is it a post hoc average of all societies , and therefore wrong in any particular society.
Joseph writes:
Hello Twivers,
I am an undergraduate microbiology and chemistry major at the University of Michigan, and I wanted to inform you of a very good interview with Wuhan Virologist Shi “Batwoman” Zhengli in reference to your recent discussion about Wuhan virology in TWIV 645. I have linked below in a recent interview in Sciencemag about her side of the story. She totally refutes the administration’s logic and reasoning about the origin of the Sars-COV-2 outbreak in wuhan.
“In her written answers to Science, Shi explained in great detail why she thinks her lab is blameless. WIV has identified hundreds of bat viruses over the years, but never anything close to SARS-CoV-2, she says. Although much speculation has centered on RaTG13, the bat virus that most closely resembles SARS-CoV-2, differences in the sequences of the two viruses suggest they diverged from a common ancestor somewhere between 20 and 70 years ago. Shi notes that her lab never cultured the bat virus, making an accident far less likely.”
Thanks for everything and stay safe,
Joey
Jo writes:
Hi Dr Racaniello, TWiV hosts, contributors and guests,
I’m a new listener to TWiV and other MicrobeTV shows (since March). After listening to TWiV #640 with Dr. Michael Mina, I’ve contacted over 300 personal contacts, elected officials and public health organizations (including all the states’ epidemiologists and all the states’ PTA offices) entitling my emails and correspondences with “Paper strips printed with monoclonal antibodies for fast, frequent, cheap testing — we CAN open our economy, our schools safely” and linking the TWiV show, the NYT opinion and the MedCram episode covering this topic. I’ve included the on-point quotes from Malcolm Gladwell and Dr. Roger Seheult from MedCram.
Even before episode #640, I’ve found your discussions so helpful that I have shared TWiV and MicrobeTV links with my contact circles. Dr. Giffin’s weekly contributions help me become both less distressed about, yet more respectful of, the consequences of SARS-CoV-2 infection.
Thank you all for your work. I suspect that there are many like me, a mostly silent but highly appreciative audience, busily learning from and sharing the information and ideas from MicrobeTV podcasts and videocasts.
Best,
Jocelyn
mom of 2
former tax consultant
certified pickleball instructor
Jon writes:
The Michael Mina episode was as you say a (potential) game-changer! It moved me to forward an email to my 40+ friends who follow podcasts, to point them all at the proposed approach. It also moved me to email my congresswoman, Anna Eshoo, who apparently is among the more receptive, to hear this message. Please feel free to add my letter (below) to your collection at https://www.microbe.tv/twiv/testing-letters/; I’m hopeful TWiV listeners + multipliers might effect change. The possibility is inspiring and a reason for hope.
Keep it up!
===============================================
A scientifically validated approach — frequent, rapid, cheap paper-strip testing for the SARS-CoV-2 virus — could turn the tide, help reopen schools and businesses safely, and avoid untold deaths and further economic misery. PLEASE, Congresswoman Eshoo, read https://www.nytimes.com/2020/07/03/opinion/coronavirus-tests.html ! The author, Michael Mina, is an epidemiologist, immunologist & physician @ Harvard School of Public Health & Harvard Med School (https://twitter.com/michaelmina_lab)
From age 18-65, I almost *never* contacted my representative; I’m determined to be heard now, because so much is at stake. The federal bureaucracy is moving too slowly, and the pandemic is ravaging the U.S. more than any other country. It’s a tragedy. It’s unnecessary. *It can be brought under control*.
FREQUENCY is far more important than sensitivity for effective testing, and is absolutely critical to enable schools to reopen safely. Dr. Mina has shown how we can do it. PLEASE help him be heard, and overcome roadblocks from the FDA. I encourage your staff and you to go deeper into the details, e.g. listen to his chat with expert virologists and immunologists at https://www.microbe.tv/twiv/twiv-640/ (“This Week in Virology”, an authoritative, long-running podcast.)
I would appreciate your directing your colleagues’ attention to these ideas. I am eager for your reaction, and for suggestions of other officials I should contact.
Thank you for your attention!
— p.s. I just called and left a message about this at your district office.
Shi-Hsia writes:
Dear TWiV team,
I’m a University College London PhD student, working with Alex Sigal at the Africa Health Research Institute in sunny Durban, South Africa. Even though we’re in the middle of winter, the temperature is a comfy 22C in the daytime. Since I’m doing my PhD on tuberculosis antibodies, I’ve found TWiV immensely helpful in trying to keep up on general virology.
I’m excited to have jumped on the coronavirus research wagon. My PI is leading a study on the early immune response to Covid in patients in Durban hospitals, and I’ve recently started doing ELISAs.
Could I please jump on your soapbox for 5 seconds? In TWiV 644, you covered the ChAdOx Phase 1/2 trial paper and there was a little discussion comparing the pseudovirus versus SARS-CoV-2 neutralization assays. They used a lentivirus-based pseudovirus, which seems to be becoming popular because of the convenience of reverse genetics systems for lentis. For listeners who aren’t virologists, lentiviruses are a genus of retroviruses that include HIV.
We received some other lentiviral reporter pseudoviruses from our collaborators in the USA ( https://www.mdpi.com/1999-4915/12/5/513/htm ). While we’re immensely grateful to them for the kind gift including a lot of other critical reagents, the lenti reporters are not working for us for a very important reason – a LOT of people here have HIV and are on antiretroviral medication, including many of our study participants. Our postdoc who’s trying to get the pseudovirus neutralization assay working has found that it’s nuked by plasma from people on ARVs.
We are going to try to get a hold of reporter pseudoviruses on other backbones such as VSV, but this may take a while. Personally I would like to do SARS-Cov-2 microneuts on a few of our samples as well to check for correlation with any pseudovirus assay.
Having a working vaccine is going to be especially important to immunologically vulnerable people, so I would hope that later trials in Phase 3 will seek to recruit some volunteers with HIV. I appeal to virologists in the “global north” to please think about the 38 million people around the world living with HIV, and your colleagues who are working in high-HIV-prevalence countries. If pseudovirus neutralization assays are going to become common or standardised, PLEASE don’t settle on a backbone that’s killed by antiretrovirals!
Best regards,
Shi-Hsia Hwa, MSc.
(my name is easier to pronounce for English speakers if you break it down as “Shih Sia”.)
PhD student, UCL
Sigal Lab, Africa Health Research Institute (fka K-RITH)
C writes:
Hi TWIV team,
It’s sunny and 88F here with a 10% chance of rain. I’ve never written in, but I’ve been listening since 2011 when I began at a little start up that was making a vaccine from CDC technology. It’s been almost 10 years since then and our vaccine is almost ready for commercial marketing submission (just for comparison to some of the well funded vaccines in development more recently, we have officially been in development for almost 30 years dating back to the first development work at CDC). Even with better funding lately as the disease of interest has taken more lives and increased in priority for global health, the development for large scale manufacturing is complicated and rushing can cause issues with transfer of knowledge as the development based manufacturing is transferred to large manufacturing plants and importantly, testing sites.
This is further complicated by the regulatory landscape which is diverse and means it is challenging to conduct large scale manufacturing and testing that suits the needs of all competent authorities in the commercially marketed area of interest and in a timely/strategic manner that is accounting for the seropositivity of the population required for achieving efficacy (eg trials must be conducted in endemic and non endemic areas) and the patient population based on the clinical protocol exclusion criteria and informed consent (I could go on and on).
This actually leads me to the reason for my letter today which is simply that the US military is not an uncommon subject pool for vaccine clinical trials that are approved by FDA. The military makes for a good subject population for early phase trials due to good adherence to the clinical protocol during the clinical operational requirements (can be included in the routine vaccination schedule for new recruits) as well as good adherence/reporting by the subject pool. One specific area of use is due to the close quarters of the population and potential to survey both seronegative and seropositive subjects (or subjects which later become seropositive and acquire infection from other circulating strains, for example with norovirus G1 vs G4 etc). The trickier areas are with respect to informed consent and clinical blinding. The military is a particularly vulnerable population and so incentive and pressure from authority figures needs to be carefully considered/planned and documented for appropriate informed consent.
Another thought on commercialization as it applies to the current environment. When we rapidly scale up the development, especially in the case where there is no defined correlate of protection, we risk missing important Quality data which can impact everything from the selection of testing methods for primary endpoints or acceptance criterial in the clinical protocol (eg quantitative vs qualitative PCR, Microneutralization with greater than 50% neutralizing antibody titers coupled with exploratory cellular immunity testing, sequencing of reversions based on injection date and adverse events reporting) to final dosage presentation form (injection versus micro injection, combination product vs 2-barrel auto injector) and pharmocovigilence surveillance based on method control trending limits and testing time points (from small R&D to large scale testing to public consumption). Companies link usage with patient history files through apps and other smart collection methods from development through beyond commercialization. The practical significance of the statistical data needs to be well understood at each stage alongside the statistical significance. Issues in understanding or design/planning can ultimately lead to serious results, recalls or market actions when the product is ultimately brought to market and tested on a much broader population than in clinical trials (for example see Dengvaxia), if it makes it that far.
When I hear the commitments to making so many doses it is staggering but not if you consider that manufacturing sites are making anywhere from 75-300,000 doses or more for one process qualification run. You need at least 3 consistent runs for most marketing applications but considering the amount of work that is happening at the same time (the development scientists reformulate and the clinical serology results change boosting use protocol or result release test) and those data need to ultimately be bridged back to the initial clinical filing and process qualification runs, leading to re-manufacture. So just because a company is making “phase 3” material, does not mean they will be ready for commercial manufacturing and just because many doses are capable of being made, many of those doses may ultimately not be commercially salable.
All of this leads me to be cautious when I hear the estimates of commercial timelines. I’ve seen a few surges in venture funding that have still not led to commercial product. Not to say we shouldn’t keep trying, but more so that we need to increase and consistently fund science in its raw form to enable better understanding of the development of mechanisms of action, processing and data collection behind the products on which we rely for global health.
I’ll stop now as this letter has been much longer than I originally intended. Keep up the good work, always. I love sharing this podcast and the papers you review broadly within my network and they have even influenced the development of exploratory clinical endpoints in some of our trials. Industry needs to be aware of good, reliable sources of data, always, but especially in these times
Kind regards,
C
Andrew writes:
Tēnā koutou Twiven.
Hello to you all from New Zealand
Long time listener here since completing Vincent’s Virology course a few years ago. I’m a software engineer working in the science arena.
You would of course all be welcome to come and live in NZ, but be aware, although we are practically Covid-19 free, have a mild climate and are relatively well governed we also sit on the Pacific ring of fire and have a difficult to assess risk of earthquakes and volcanoes.
Having successfully pulled up the drawbridge and isolated the country into a ‘bubble’ of 5 million people I am wondering how you see this working out in the long run, unless a vaccine shows up might we see other countries reaching, if not population immunity, at least a plateau equilibrium of infection rates. This would leave NZ behind in a type of pre-covid state whereby were I to visit the US I would be more likely to get an infection or would get one more seriously.
I’m curious whether there is a situation in which many people have been exposed to levels of the virus that are too low to create a full infection. Is it possible to develop any kind of immune response that might cause later infections to be handled more swiftly and thus generally ‘damped down’ in the exposed population. Then would we see more serious infections arising in a naive population. I’m not explaining it well but I’m imagining an effect such as when the new world populations were first exposed to European diseases.
Thanks for your high standard of convivial, erudite conversation.
Andrew
PS. When you have a chance to do a non-covid episode I would like to hear more about viruses – the kind that don’t make you sick. I understand there are many of these and would like to know more about them.
Eileen writes:
Dear TWIV,
Thank you for all the work you do to help people like me understand more about virology, epidemiology, and immunology. A friend of mine from Spain, who is much more informed and credentialed than myself, told me to listen to you as I started spinning out about the coronavirus in January. I have learned so much from your podcast, and I appreciate the work all of you do and all who have come onto your show (especially Dr. Griffin and Dr. Fauci, both of whom I’ve become huge fans of).
I have thus far avoided being infected. However, my friend in Spain unfortunately did not. While he has since recovered, I am a high school teacher outside of Chicago headed into a schedule of essentially a full face-to-face classroom of my students in two weeks. While seeing them again does my heart good, every other part of my body which has any understanding of biology is incredibly terrified at this prospect. I despise the coronavirus even more because of the position I am now in along with so many other educators this fall.
I want to pivot away from that and concentrate on what I can control: what is being taught in my classes. I teach biology, genetics, human physiology and a medical chemistry course. While I have taught a big picture level about the immune system previous to this, I feel like the more I listen to your podcast, the more I realize I am really more underprepared than I originally thought to do so at any level of detail. I want to be able to teach about the immune system in a more detailed way that works for various levels of students I teach that are from 14-18 years old. My intent in one of my classes is to wrap the systems that I teach around those that are most affected by the virus and the viremia of coronavirus. There is so much misinformation that my students are regularly subjected to and I feel like it is my mission to help students not only understand this virus correctly but also be more informed about the nature of science. But, I do not want to be the cause of any of their misunderstandings or further cause confusion for them.
Therefore, do you have any curriculum or resources that you think can capture the best way to explain immunology in a way that is ‘succinct and simple’ while connecting it to coronavirus? I know this probably seems like an oxymoron and ridiculous because from listening to your podcast, I realized immunology is anything but that, but I feel like what I have been doing in my classes isn’t good enough.
I have seen your Virology 101 resources, and I appreciate those. I was hoping your group may have aggregated resources for teachers, specifically high school teachers, that maybe I have not seen. Ultimately, I want to be able to prepare a group of students with information to excite them about and incite them into this arena of science so we can have a generation of people prepared for the next big one (hopefully long after I have retired:)
Thank you again,
Eileen*
*Currently sunny and clear, 70 degrees F, 21.1 degrees C in Arlington Heights, IL
Chris writes:
Hi TWiV,
Thank you for all that you are doing during this time. Your take on the current situation has been very valuable for me and the people I know.
Here is my question:
Given the massive spread of SARS-CoV-2, what is the risk of recombination with another Coronavirus to produce another novel human virus (i.e. this may occur during co-infection of a single host with multiple Coronaviruses)? And, also, is this a concern? Why or why not?
I study bacterial viruses, where this is common, but I know nothing about this phenomenon in eukaryotic viruses.
At this point I have not heard you address this concept, but my apologies if I missed it.
https://www.nature.com/articles/nrmicro2614
Best,
Chris
Rich writes:
Dear Twivs–
It’s 68°F here in Boulder Creek, California, and feels like 78°F, on its way to a sunny 87° today. With a hopefully low chance of Covid-19.
Masks can block lots of the infectious particles, either as droplets or even aerosolized. If it’s true that the dose of the infectious particles that one is exposed to relates to the severity of the disease that one experiences, then the question is whether one should wear a mask at home to limit the impact severity on oneself from exposure to others in the household.
I can’t imagine doing this, but it kind of makes sense to do. On the TWiV podcasts, none of you are wearing masks, but neither do any of you have others in the room.
What’s your thinking about this?
Theoretically does it make sense to wear a mask at home? And, do any of you?
PS: I’m “just” a retired computer programmer.
Yours Maskfully,
–Rich
Justin writes:
Hey team TWIV,
I ran across a seemingly plausible article saying that the anti-depressant prozac was found to suppress the replication of SARS 2. To quote from this article,
“To test cytotoxicity, Vero cells were incubated with the agents for three days and then checked for cell growth. After incubating the cells with increasing concentration of the drugs, they were then infected with SARS-CoV-2. The concentrations of fluoxetine were close to the 0.8 µg/ml dose currently used in the treatment of depression.
After three days, viral RNA was extracted, and viral replication was quantified by real-time polymerase chain reaction (PCR). The team reports that the 0.8µg/ml dose of fluoxetine was effective at inhibiting SARS-CoV-2 replication.”
This sounds significant! Is the inference from this experiment to real world SARS infections sketchy? Can team TWIV tell me and other interested listeners whether Prozac users should take some comfort in these results?
Best,
Justin
Here is the journal article which I dont have access to: https://www.biorxiv.org/content/10.1101/2020.06.14.150490v2
Suellen writes:
Hey TWIV team!
Thought I would forward this email from one of our neighbours here in Roswell, GA. He’s a busy guy, but maybe he would agree to give a quick update on TWIV if you asked him.
As you can see, things have gotten pretty bad here in Georgia. The hospital this doctor works at is in an affluent area, so imagine what’s happening at places like Grady Memorial.
And, yeah, we are the state where the governor is suing the mayor of Atlanta because she’s mandating masks, and he sees that as an infringement of our liberties.
I have to say that I was heartened when I went to the local Kroger yesterday and saw that everyone was wearing masks. Now, Kroger and other businesses have mandated masks, but I was hearing that people were walking in wearing them and then taking them off. Yesterday there was none of that — people were masked up and being more conscious of personal space than I’ve seen in the past. So maybe despite our governor, we are getting the message here.
And a quick add — as you guys know, I’m an avid horse person. Well, I have been to three horse shows during the past month or so, and I do have to say that they are adhering to the mask rules and managing to keep people safe. This is a big thing, because a lot of people rely on horse shows to make a living — horse trainers, judges (horse show judges, that is), breeders, etc. It’s a big industry, and if you can’t get out there and show you can’t really make any money. So I’m proud of our horse folks here in Georgia, who despite mostly being pretty right-wing (I parked next to a truck yesterday at the show at Chattahoochee Hills that had a decal on the back window saying “All Aboard the Trump Train.” Yeah, you can’t make this stuff up) anyway — despite being pretty far right, they are managing — with some grumbling — to play by the rules set by our governing bodies and MASK UP.
So maybe there is hope for us after all, but it’s going to get worse here before it gets better.
Suellen
Roswell, GA
Hello neighbors,
I’ve just finished my 7 days in the ICU and I figured I would share my observations with those that are interested.
I wanted to start by sending well wishes to our neighbors who have tested positive. I hope you all are doing ok and please reach out if you need anything, even just to talk.
Any ways, here goes.
– Last time I was on service, I was worried that our numbers were growing. That only got worse. This is a snapshot of our covid census as of today.
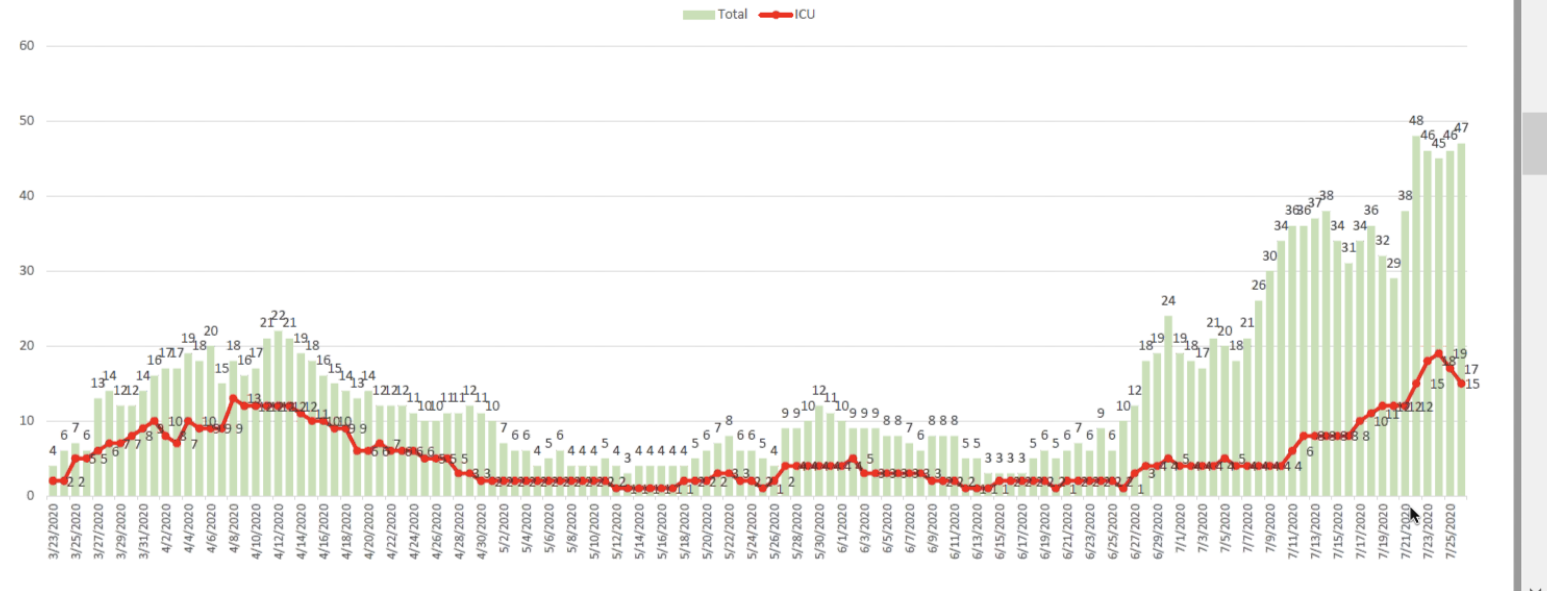
– We are sitting at 47 total COVID patients with 15 in the ICU. Two days ago we were at 19 in the ICU. This is a 24 bed unit. Our unit is full and has been full for the last 5 days. Our secondary ICU which we opened up is also at capacity with non covid patients. We have a COVID floor for non ICU patients, and this is full as well. Hence we are now having to place COVID patients in floors with non COVID patients.
– These last few days were heartbreaking. With a full ICU, we have been on diversion many times. This means that sick people from the community who need an ICU can not come to our hospital. The ambulances have to go somewhere else. This means that instead of focusing on the very sick people in my unit, I had to go to the floors and manage patients there without all the ICU resources, because I didn’t have beds to bring them down to me.
– Most COVID patients are spending between 7-12 days in the unit (compared to 2-5 for an average flu or pneumonia). This means we will have a very hard time making room for more patients
– We lost 4 lives to COVID in the ICU this week. 4 lives too many.
– Our nurses are tired, overworked, asked to pick up shifts on their days off. They are being tripled. This means instead of 1 nurse for every 2 patients, the ratio is 1:3.
– Ages ranged from 27 to 80s. Younger folks are not less sick, some younger folks are incredibly sick.
– We are short supply on testing in the hospital, short on Remdesivir (antiviral medicine) and the blood bank is extremely low on convalescent plasma. Please, if you know someone who has recovered from COVID, encourage them to donate blood.
– Please know that our medical team is working hard to help those who reach us, but we need lots of help reducing the amount of folks who do. We feel that we are running out of ways to care for those in need. Please. Wear a mask.
Stay safe,
Ed