
John writes:
Hi Twiv!
I’m wondering if I can make a request. My wife’s name is Amy and she is one of your biggest fans. She’s a physician and listens to your podcast religiously. She tells all her friends about you. She has the Twiv to-go coffee mug and the sweatshirt and the regular coffee mug and the tote bag. (So do some of her friends because she buys them as gifts.) At some point last year you read one of her letters about your podcast being Covid-porn and it made her month.
Amy volunteers to lead the COVID committee at our daughter’s preschool in Lincoln, MA (LNS what what!) With weekly zoom meetings, weekly testing (first individual, now pooled) and constant emails and updates to protocols and procedures, she and her fellow committee members have worked countless volunteer hours helping to keep the community safe. We’ve made it the entire year without having to close once.
On May 11, Amy turns 40. It would make her day if you could wish her a happy birthday on the podcast. I know that listening to you each week has helped her make it through this pandemic and in turn helped keep our school and town safer. It would mean a lot.
Thanks so much for all you guys do.
Best,
John
Jens Kuhn writes:
Today I listened to #750 and had a few minor thoughts:
Cattle vs cows. The species is Bos taurus Linnaeus, 1758. The standardized vernacular name for the member of this species is “aurochs” (Wilson & Reeder Mammal species of the world, 3rd ed.). My understanding is that “cattle” refers to domesticated and likely interbred aurochs populations, i.e., cattle is much more an agricultural (similar to “swine”) than a zoological term (such as “domestic pigs”). Once you go down that road: a cow is not just female cattle: it also needs to have given birth. Females that have not given birth under 3 years of age are called heifers and all kinds of other fun names are used for other females that make foreign English learners want to jump out of windows. So, yes, stick to cattle as long as the animal is not “wild”
The name Lloviu virus is derived from the name of a cave in Spain. The “Ll” is therefore pronounced “ye”: yov-yoo or yoh-vyou
“Mortality rate”: mortality is a rate by (epidemiological) definition, so no need to say “rate”. However, mortality is defined as number of deaths per number of apparently health population (typically, I think, per 100,000 health population) per time frame. This means that the mortality of Ebola virus disease is very low. The case-fatality rate = lethality is the number of dead per number of sick. This means that CFR = lethality of Ebola virus disease is concerningly high.
Glad to be back 😊
Jens
Carson writes:
Hello TWIV!
I’ve been listening since the pandemic started and love your content, knowledge, and everything you share! Thank you for all that you do! I’m just a small business owner/software developer from Englewood (next to Denver, CO) where it is currently sunny and beautiful at 34 degrees F.
I am wondering why someone with proven natural immunity to SARS-CoV-2 through a documented infection, who successfully and quickly recovered without any lingering effects, without any comorbidities, with a strong immune system, etc. would or should consider taking one of the vaccines?
Why would or should someone with this experience/status take on the unknown potentially negative long term affects of one of the vaccines on top of the unknown potentially negative long term effects of having had COVID-19?
I ask this especially in consideration of the peer reviewed study that shows that natural immunity has been shown to be effective against all of the known variants:
Reuters article about the peer reviewed study:
The study the article refers to:
https://academic.oup.com/ofid/advance-article/doi/10.1093/ofid/ofab143/6189113?searchresult=1
Is there/are there any studies that explain why someone with this history should consider vaccination?
Thank you for any insight you can offer!
Ryan writes:
Dear Microbe.tv podcasts I have mentioned vaccine debates in the past but had no idea the impact is way bigger than I was thinking back in 2019. Now the state of Connecticut has passed a vaccine law similar to California’s SB276 and SB277 removing non medical exemptions to vaccines. Yes it’s poignant given the impact of the SARS-COV-II pandemic of the past year.
Gregory writes:
Dear TWiV,
On a recent TWiV, Vincent claimed that George Gao, the head of China CDC, had said that CoronaVac is only 50% effective. This is wrong, but I don’t blame Vincent – this issue has been widely misreported in the media.
George Gao did not make any claim about the efficacy of any particular vaccine. He certainly did not name a specific percentage for any vaccine. He gave a talk at a conference about vaccines, and in one of his slides, he gave some general thoughts on how to improve the efficacy of vaccines with “not high” efficacy. He did not name any specific vaccine. He said that one can try modifying the schedule of the second dose or using a different vaccine for the second dose. He also praised mRNA vaccines.
George Gao’s slide was seized upon by someone at a think tank (the Council on Foreign Relations), who claimed that George Gao had “admitted” that Chinese vaccines don’t work (https://twitter.com/YanzhongHuang/status/1380885689575817218). This spread like wildfire in the media. Even the BBC misreported this story. George Gao gave a subsequent interview in which he said his statement had been misrepresented (https://www.globaltimes.cn/page/202104/1220774.shtml), but few in the Western media seemed to care.
My interpretation of this entire affair is that the Council on Foreign Relations cynically wanted to score geopolitical points by dunking on Chinese vaccines. Unlike the United States, which until a few days ago had exported almost no vaccine doses, China has exported nearly half of all the vaccine doses it has produced so far. Painting Chinese vaccines as somehow defective is a convenient way to negate any image gains China might make through its more generous vaccine export policy.
Aside from misrepresenting George Gao’s words, two things went missing in the media coverage of this story:
1. There are several Chinese vaccines. Sinovac and Sinopharm have each developed inactivated whole virus vaccines. CanSino has developed a single-dose adenovirus vector vaccine. Anhui Zhifei Longcom has developed a protein subunit vaccine. They have different efficacies. They’re all “low” by the incredibly high standard of the mRNA vaccines, but some are similar to AstraZeneca and J&J vaccines.
2. “Efficacy” can mean different things. What endpoint are we talking about? Prevention of mild symptoms? Prevention of serious disease? Prevention of death? (I recall that Alan Dove raised this point.) There’s a serious worldwide shortage of vaccines right now, and a vaccine that reduces chance of serious disease or death by an order of magnitude will still make a huge difference.
I love your show, but I just want to correct this one issue.
All the best and thanks for your hard work in putting together episodes week after week,
-Gregory
Greg writes:
Salutations Twiv Team,
It’s 72 degrees fahrenheit in Ha’iku, Maui. My wife and I are both vaccinated (she’ll get a second shot of the Moderna in a little over a week) and so are the 3 grandparents in our bubble – as is my father in Utah. What a relief! I’m just coming out of a kind of honeymoon glow – now it’s time to think about the rest of the world and that includes my kid.
We’re eager to get our nine year old daughter vaccinated asap – looks like we’ll have to wait a while. Given the recent news about breast milk containing antibodies to SARSCoV2 in JAMA, https://jamanetwork.com/journals/jama/fullarticle/2778766
we wonder, can she be effectively immunized by drinking breast milk from a vaccinated, nursing mother? If so how much mookie would confer the effective dose?
Sincerely,
Greg
PS, since I have just referenced an article from Israel I want to raise the issue of vaccine injustice in Gaza and the West bank. As I understand it, Palestinian workers in Israel are being vaccinated but the partially-recognized and blockaded State of Palestine has only been able to secure doses in the tens of thousands for a population of over 5 million people. Your conversations on TWiV have regularly touched on the Isrealli vaccination program but you’ve skirted the issue of injustice across the barrier walls separating Israel from the majority of the Palestinian people. I’m sure I’m not the only listener to point this out. Please bring back that feeling we got when you paused from virology to show solidarity with the Black Lives Matter movement over the summer. Your work gives hope to many people and I call on you to let that blossom further than the various barriers to public health internationally.
—
Greg
Kahului, HI
Tamar writes:
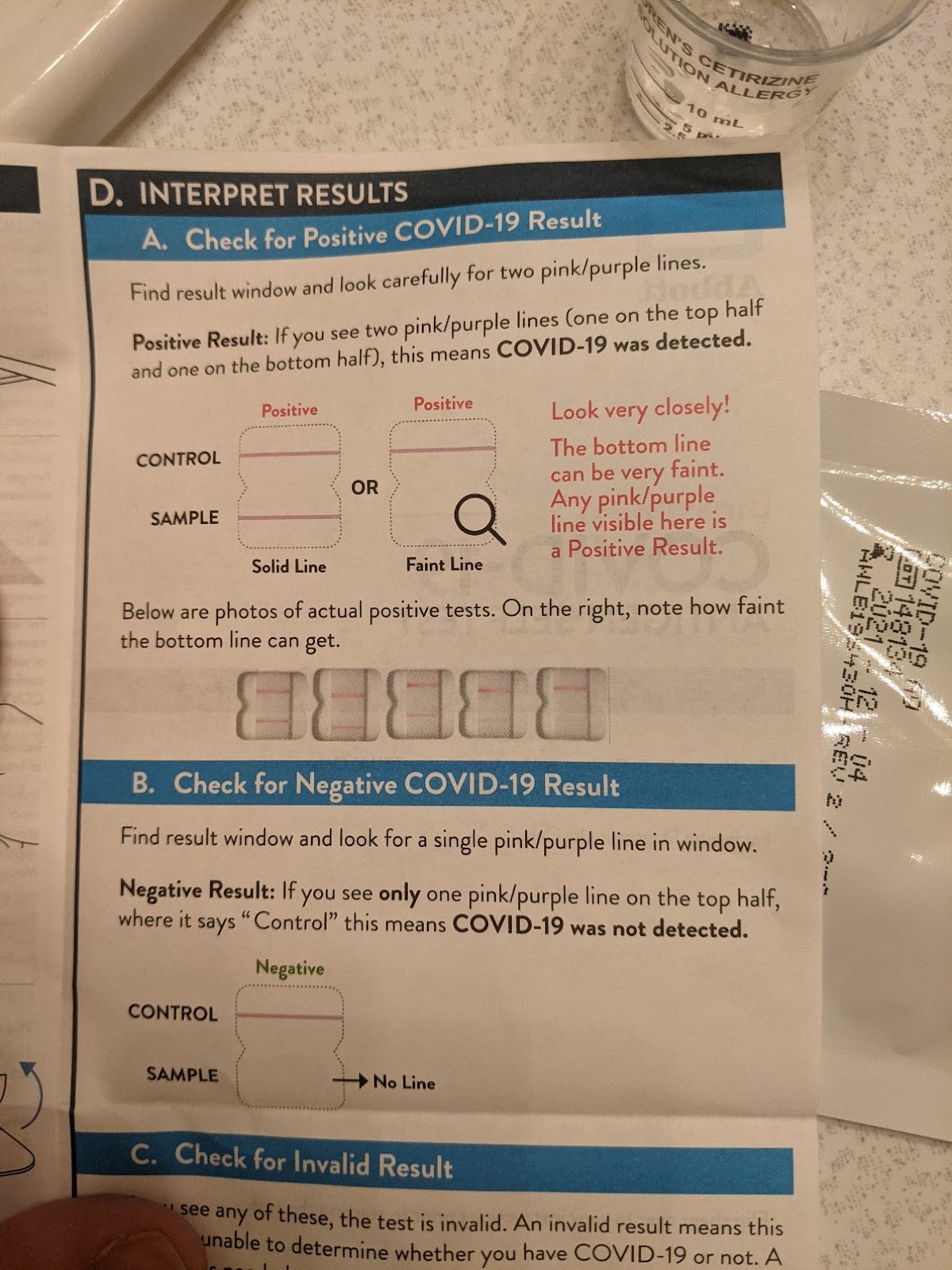
I got to use the new Abbott BinaxNow rapid at home antigen test on my elementary school kid who had a sore throat this morning. Instructions were clear and it was easy to do. And she was negative (which I figured was the case but had to double check before sending her to school).
For $10-12 per test it’s totally worth it. So happy to have this option even though we (thankfully) have free PCR tests here in Nebraska with a <24hr turnaround. And I definitely preferred using an anterior nares swab on my kid vs making her get an NP swab.
Best,
Tamar
Haley writes:
Hi TWIV!
I’m a long time listener of your podcast, and really appreciate the work that you guys do to inform the public about all things covid. I have a question about post-vaccine long term effects that I’m hoping you guys could help me understand.
I got both doses of Pfizer (dose 1 March 23rd, and dose 2 April 13). After each dose, I experienced all of the usual side effects, but they lasted for about 2 weeks. After dose 1, I got a migraine that lasted almost 10 days, and I was so fatigued that I couldn’t get off my couch. Symptoms improved for the most part before dose 2, but I’m still dealing with almost daily headaches and muscle/ joint pain in my legs. I haven’t been able to exercise or live daily life due to this pain, and doctors don’t know what to do. I’m all for vaccination, but as a 26 year old woman, I regret getting the vaccine. I feel it’s done more harm to my body than good.
I’ve seen this type of thing reported among young women on other social media forums (although I take these reports with a grain of salt). Is there any data from the trials or real world that could give us an idea as to why this happens? I would also love if you have any thoughts on what I could tell my doctors about how to treat me. This feels like long covid from a vaccine. 🙁
Please help!
Haley