
Sheela writes:
Hi TWiV Team,
I have been listening to TWiV and Immune for about a year and am still working my way through the fascinating back episodes. I love the podcasts as well as the Columbia BIO 4310 and Dr Barker’s Immunology course. I do not have a science background, and now wish I could go back 30 years and study virology and immunology formally.
I feel like I am not understanding something properly in episode 725 with Drs Eva Harris and Janet Smith. Dr Harris says that the secreted NP1 protein of dengue itself can cause vascular leakage. (She says that there is a lot of conserved sequence identity among many flavivirus NP1 structures, so not sure whether they have same effect.) However, much of the rest of the episode discusses using this antigen to create a vaccine.
I know that other subunit vaccines can be made with a particular antigen just because it has epitopes that gamma globulins can bind to block infection, but they do not themselves cause pathogènesis, but act more as “heralds” if memory B or T cells encounter them in a viral invasion after vaccination. However, Dr Harris said that NP1 alone was essentially a viral toxin that causes immune cells to release vasoactive cytokines, starting a cascade that results in breakdown of the endothelial barrier.
If this isolated antigen is so pathogenic and destructive, how can it be used as a subunit vaccine? Is it just that it would be used in a very small amount? I don’t recall any discussion of changing any amino acids on it to make it less pathogenic, but preserve immune system recognizability.
I cannot figure out what I missed in this discussion.

Thank you so much for your wonderful work. I listen all day while walking my dogs (of course!), doing housework, and driving.
This is a photo of one of my dogs sleeping during episode 60 (Making Viral RNA) which I am playing and re-playing to try to fully understand. I guess he doesn’t find it as fascinating as I do!
Thanks,
Sheela in Silicon Valley
Cheryl writes:
TWIV is a very special asset. Enormous gratitude for your efforts.

Susan writes:
Hi Vincent –
Thanks for all your work in fighting the scientific ignorance that, at times, really feels like it’s taking over.
I’m an engineer by (over) education, but a scientist at heart. I took Genetics 160 from Rayla Temin back in ’91, but that was about it for my biological science background until now. Like so many people, I’ve found the mainstream coverage of the pandemic to be … let’s say “wanting”. Your lectures, podcasts, and live-streams are a great way of filling in the gaps (and learning cool stuff too).
In one of your podcasts, you were lamenting that you aren’t reaching that many people. As someone pointed out at the time, your influence goes beyond just those who tune in directly. I, for example, am a senior board member of the local recreational ultimate frisbee organization, and your podcast helps me to make decisions about how and when to restart our athletic leagues. Our league is one of the largest in the country, so you can add our 4000 or so participants to the list of people you’ve affected, indirectly or otherwise.
Keep up the good work!
Best,
Susan
p.s. I ordered the TWiV tote bag, but I have no idea how big it is. I suggest adding the dimensions to the product description.
Scott writes:
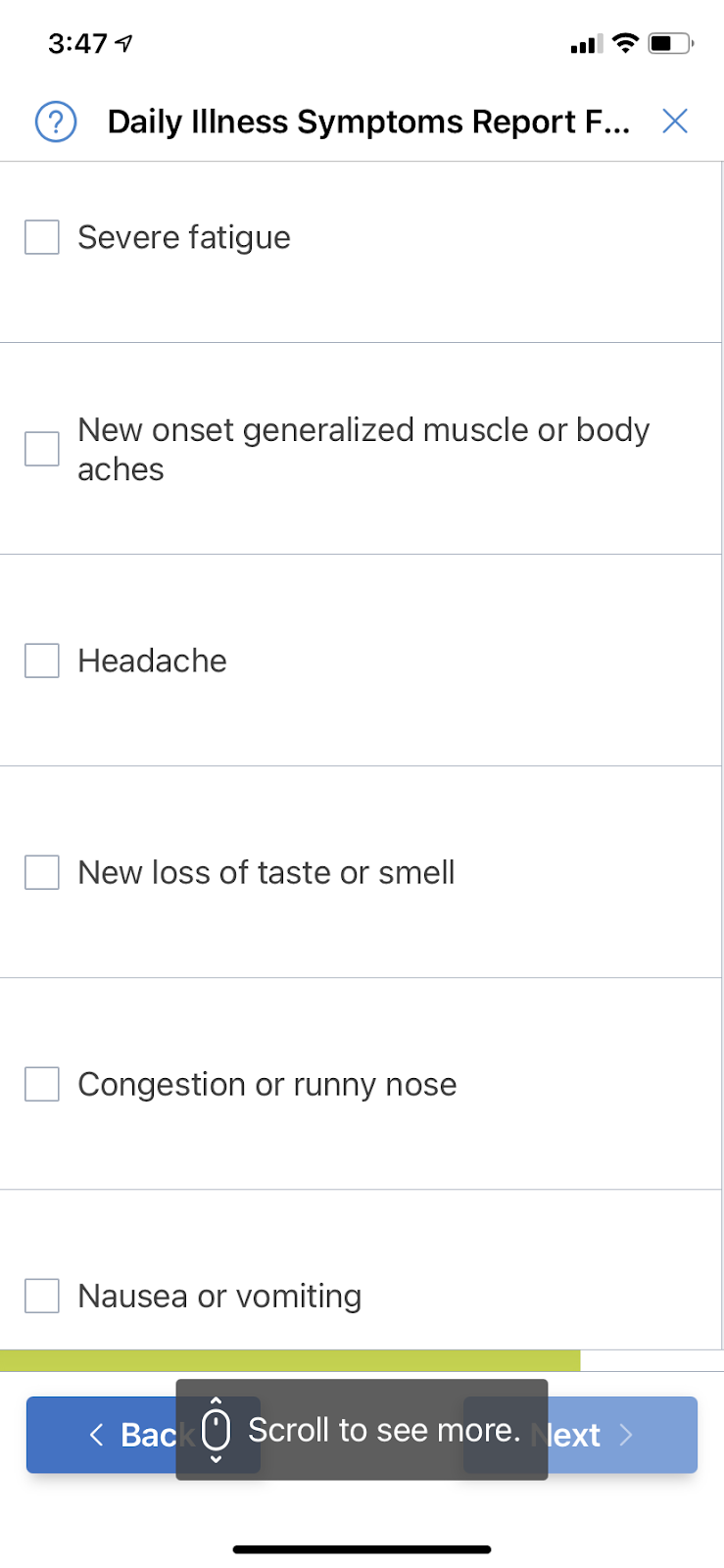
Hi all. Love your podcast. In an episode this week someone asked about the trials and the questions asked, relating to taste and smell. Below is the daily symptom report form for Novavax.
Ivan writes:
I wonder if you and the group could comment on a few things.
1) I enjoyed your discussion of the NEJM article on the COVE study of the Moderna vaccine including the discussion about same arm/opposite arms for the boost. The question of germinal centers in the local lymph nodes vs elsewhere etc. When I read the paper last night, I noticed that (on page 495) the study protocol was that the second shot would be given in the same arm. I didn’t see data reported regarding compliance with this and I noticed that same arm is NOT part of the CDC instructions. I have volunteered at the vaccination site set up by my hospital and there was no directive to give the boost in the same arm. Intuitively I would choose the opposite to try to minimize local side effects unless that adversely impacted efficacy. I don’t know that it does but since we are trying to adhere to evidence-based practice, it is fair to say that the same arm works, We don’t know if opposite arm does. Right?
2) In a recent episode of TWIV there was discussion (banter?) about making vaccination involuntary. I think Dickson may have said something about criminalizing refusal. I am all for vaccination(s). But it seems to me that the threshold of evidence for safety has to be very very high before you can consider that extreme step. Don’t get me wrong, I am promoting it as a doctor and as a medical director and as a parent and as the child of elderly parents etc. But, even the FDA panel that approved the EUAs did not do so unanimously. Before you lock up lay people who are hesitant, let’s address the concerns of the 2-3 scientists on the panel who voted no. That might be an interesting discussion for TWIV. I doubt these are anti-vaxxer kooks.
3) I try to be evidence based and I appreciate Dr Fauci and others who point out that we don’t have much data regarding efficacy of a single dose of either mRNA SARS CoV2 vaccine. Saying the “curve is flat” for 12 days is far from conclusive. As Brianne essentially said, the protection from one dose MIGHT fall off a cliff X weeks after administration. BUT I doubt it. On the other hand, vaccinating half as many people is almost certainly really bad. Therefore, I agree with the “British approach” to emphasizing the first dose in the population. If we can get 100 million people 1 dose that is very likely to be better than getting 50 million people 2 doses, at least in the short run. We are not saying never give the second dose. But let’s leave fewer people without any protection. If it turns out that one dose is not durable, we will begin to see it and we can change course. Everything I have read about boosting (which is a lot less than you guys have read) is that there is a MINIMUM wait of 3 weeks. There is no mention of a maximum wait. I am sure that exists in theory although >10 years for Tdap is standard. I know there is minimal data for waiting longer than 21 or 28 days. But those intervals were selected (I think) to try to get the study done quicker, not because they were likely optimal. I think the British approach makes sense in a pandemic. In an emergency you sometimes have to shoot from the hip.
4) The other guidance I find confusing is ignoring previous infection in considering whom to prioritize for vaccination. I had the disease in March. I had a high titer of S Abs by the Mt Sinai (NY) test and I donated plasma. In the context of a shortage of doses, I think it is unethical for me to get the vaccine when there are others who are not immune. There is no question that we see re-infection. Some of what we think is re-infection is not, as you have discussed at length on TWIV. But some is. Anecdotally, what I see in the ED is way less than 5% of people even though some may have had undetected primary infection which would make our estimate lower than the real number. I certainly cannot give you a precise number but every one of my colleagues I have asked would peg the number way below 5 % which is the “failure rate” of the two mRNA vaccines with EUA. Therefore natural infection is likely more effective than vaccine which is almost always the case, right? So it looks like a duck and it quacks like a duck. It’s a duck. If there is a shortage of vaccine, emphasize the people who have not had the infection first. I will get mine when everyone else who is willing has had theirs. Sure, my immunity may wane. But so might it wane after vaccination. My Mt Sinai Ab titers may be lower now. They almost certainly are unless I have been re-exposed. But that is what is supposed to happen. Memory B cells and all that jazz. Basic science. Also, in my world, titers are a proxy. What matters is disease.
5) Antibody tests. We have the Abbot IgG test in our lab. The is to the N protein. For some reason, even though I was PCR positive and with a high IgG titer vs S at Mt Sinai, I was negative 3 times by Abbot. My lab director ended up getting my serum tested by other platforms and I was positive for S by several others. I was reported to the FDA as an Abbot failure. I know you spoke recently about being able to differentiate natural immunity from vaccination by using N vs S abs but it is worth noting that we really don’t know what the sensitivity is of these tests. Numbers are quoted but you tell me a good gold standard given the enormous rate of asymptomatic infection, and I will stop pestering you…
Thanks again for your service (to me and to the world of knowledge)
Ivan
Ivan T Miller MD FACEP
Medical Director,
Department of Emergency Medicine
Westchester Medical Center and
Maria Fareri Children’s Hospital
Carla writes:
I have never done well in my science classes except social science, but the COVID crisis took me to TWIV at the beginning of the pandemic. I listen to almost every word but sometimes have to tune out when it gets too technical.
I’m a clinical social worker and a tennis player as well as the wife of an 81 year old, though I’m much younger.
We live in Utah so are indoors for tennis in the winter. I chose Monday at 7:30 a.m. for bubble time for tennis, thinking that virus would be lowest since the bubble closes at 3:00 on Monday. Now I’ve been thinking, what happens to virus that’s been aerosolized if it doesn’t make it into a host? How long does it stay around? When can it be kicked up by a fan or people moving about and get back in the air?
Mary writes:
Hi TWIV team,
I thought you might be interested in these UK challenge trials that will start soon.
I know that you have talked about the ethics of these trials and wonder if you are still feeling the same about them?
Thanks again for everything you do.
Mary (part time veterinarian in Ottawa, Ontario where it is currently -18 celsius, -4 fahrenheit)
Niall writes:
Hello Twivers,
You may have touched on this before but i’m curious if biological, as opposed to intellectual property, constraints apply to the resulting efficacy when multiple vaccines (and types) are combined to “hedge your bets”.
…in case i need to clarify: I mean in a single shot, like MMR.
Still delighted to have discovered you all.
—
Niall
Jesse writes:
Dear TWiVicionados,
I’ve been a participant in the Moderna Phase 3 trial since last June. It has been very interesting. Recently, as you’ve heard from other participants, the trial coordinators and Moderna have offered participants the chance to be unblinded, find out which group they were in, and if placebo, receive the actual vaccine.
I am choosing to remain blinded, for several reasons, including:
-I’m pretty sure I got the vaccine, based on the reactions I experienced
-Whichever group I’m actually in, it wouldn’t change my life much, since my wife probably won’t be vaccinated for a while and I wouldn’t want to take the chance of spreading SARS-CoV-2 to her by engaging in risky behavior
-It’s better for the long-term trial science for people to remain blinded
However, the people running the trial at my local site keep bugging me to get unblinded! I just had my six-month check-in last week, I asked if I was the only one still blinded, and they said yes! (I’m assuming that’s only my site, but who knows.) I guess I can’t really blame people for wanting to make sure they have the vaccine as soon as possible, but still it’s a little disappointing. It seems like there’s not much point for me to be the only one still blinded. What do you think?
Thanks for all you do,
Jesse
Amanda writes:
Hey Twivers, I am in a slowly warming Arkansas (it’s been below 0 C for days, but now the temp is up to 10 C and thawing). I have a story similar to the one Paul Offit shared. I’m a clinical pharmacist, and I’ve been helping to vaccinate and giving vaccine advice. A friend called me a few weeks ago and asked for my advice about her 92 year old mother. She had booked her a vaccine appointment, but told me she was unsure since her mom had Alzheimer’s, was homebound even before COVID, and had some renal issues going on. She said she had a call to her MD, but they wouldn’t call her back. I told her I would wait on the vaccine, because there was no sense in the mom getting out, and that she should try to get vaccinated herself as a caregiver and practice the safe distancing and masking that she had been doing. She agreed. She said she would take my advice and cancelled the appointment (her MD eventually called back and advised her to wait until Spring too). The mom died the following week from organ failure. Had she kept that vaccine appointment, she would have been included in the “vaccine related death” statistics, and her daughter might have never trusted vaccines again. To be honest, I would have felt horrible too, and maybe blamed the vaccine myself. It’s hard to convince yourself with data when the anecdote is someone you know.
I’ve been sharing this story with all my colleagues who say “but what about the deaths in Norway?” When you look at a general population of fragile older folks, some are going to die whether we vaccinate or not.
Keep up the good work, love the show!
Amanda
Karen writes:
Dear TWiV
My New Year’s resolution is to send you a long-overdue THANK YOU! for all that my husband and I have learned from you this past year and for all the pleasure of listening in on your shoptalk.
Please take these 4 items as standing in for a whole bundle of things that have captured our attention.
1) May I offer a correction to Dr. Griffin’s comment on water-soluble vitamins? (https://www.microbe.tv/twiv/twiv-669/ TWiV 669, October 4, 2020, minute 18:44.)
I learned the hard way that the Goldilocks Effect applies to Vitamin B6 — if you take too much of this vitamin, the excess does not get peed out. The experience prompted this (peer-reviewed) essay:
Karen Reeds, “Vitamin B Complexities”
remedianetwork / H-Nutrition March 4, 2019 /
Part of the series, ‘What Should I Eat? Why?’ commissioned by RemediaNetwork in collaboration with H-Net Nutrition by series editors Kristen Ann Ehrenberger, MD, PhD and Lisa Haushofer, PhD. https://remedianetwork.net/2019/03/04/vitamin-b-complexities/ [most direct link], or
https://networks.h-net.org/h-nutrition
2) Thank you for the conversation with Robert Fullilove (TWiV 655, August 20, 2020). I had the good fortune to meet Bob decades ago in Berkeley. His insights and methods for raising the graduation rates of African American students at Cal (by helping them form study groups) continue to influence the way I mentor high school kids in Trenton in science.
3) Thank you and fellow TWiV addicts, Gina and Joe, for the Listener Pick (TWIV Episode 681), Covid Fan Tutte https://www.youtube.com/watch?v=LwNz8C33JOc&feature=youtu.be
We are helping it go viral.
4) Thank you for introducing us to the co-authors of Principles of Virology, 5th ed. (TWIV Episode 662). I gave the text an odd kind of plug on a listserv for historians of the book — see below. (By the way, my Princeton Research Forum colleague, Joan Goldstein, interviewed Anne Marie Skalka on “Backstory,” Princeton Community TV, https://vimeo.com/488606002. At minute 16, Dr. Skalka deftly used the book’s cover picture to explain the workings of antibodies on the viral spikes for a lay audience.)
Stay well — we need you!
With continuing thanks,
Karen
Karen and Jim
Princeton NJ
PS A gift for the parasitologists: drawings of Entozoa by Dr Thomas Spencer Cobbold (1828-1886), from the Linnean Society of London’s collections
https://www.linnean.org/news/2021/01/25/thomas-spencer-cobbolds-drawings-of-entozoa
A listener pick: Around the corner from Dr. Barker’s Drew University lab in Madison NJ, the wonderful little Museum of Trades and Crafts has mounted this exhibition: Cholera to COVID-19: Epidemics, Pandemics, & Disease. I haven’t been able to visit, but part of the show is online at https://www.metc.org/cholera-to-covid-19/#1490886705266-0512c331-5d3f
Lizabeth writes:
Dear TWiV crew,
First, I’d like to say how thankful I am that you’ve been broadcasting so much accurate information about COVID-19 over the past year. I wasn’t a listener before the pandemic started, but I do teach classes on disease outbreaks (I have a BS in Biology and a PhD in Medieval History) so your podcast is a perfect fit for my teaching and personal interests.
While listening to a news podcast today, I heard this song played during one of the commercial breaks. I played it for my husband, and he (having listened to every TWiV show for months now) said I should send it to you as he hadn’t heard you mention the song. I hope you enjoy it as much as we did.