
John writes:
Comment regards Vincent’s TWIV Disarmingly Cantankerous Rant
Hi all:
Excellent program. I am not a virologist, instead I am a retired engineer/physicist with some experience in the field of operational research.
[I love your program even though I get lost in some of the in-depth biochemistry discussions.]
In his rant at the 25-minute mark of TWIV 696 Vincent says:
“the science in public health was not applied properly”
“the job of a government is make people educated and healthy”
We are all struggling to find a sensible way forward in this pandemic.
Under the present circumstances, politicians and senior decision makers are faced with classic “multi-criteria weighted-decision-making” problems.
While I am no supporter of your president /WH staff, those in charge must consider many factors when making tough decisions like lockdowns or enhanced public health measures.
To be fair, you must acknowledge their challenges (which I am sure are not always purely politically motivated).
The TWIV panel quite rightly views the pandemic through the lenses of virology and epidemiology.
This is what you have been trained to do and you do it well.
You must ask yourselves what other factors play into the decisions being taken at senior levels.
Certainly this is a deadly disease, and public health measures will help contain it.
Listening to the rigorous virology underlying public health measures is a critical component.
But is “the number of lives saved” the key metric at play?
I would argue that to many in the Public Health arena would answer yes to this, for the simple reason that this is what they are trained and paid to do.
They cannot really say otherwise.
But as you know, there are many other equally serious issues at play – issues that do not figure directly or immediately into the metrics of fatality or long-term secondary medical effects of Covid
Here are some:
(1) the health care system itself depends directly on the continued supply of health care workers, food, drugs, materials, water, energy, specialist technicians, computers, networks, transportation, etc in an impossibly complex dynamic international web of interactions (ask yourselves how long a hospital would stay open without a chlorine supply, and how does that get to the hospital?).
A supporting economy must stay running or there would quickly be no vaccines, nor ICUs.
(2) the misery of unemployment and child poverty/abuse caused by the shutdowns is real, but misery as part of Public Health cannot be captured as easily as infection mortality rates
(3) the long-term effect of closing schools and slowing the education processes in our children is not easily measured, but certainly damaging to the nation long-term
(4) the permanent closure of businesses will affect the long-term prosperity of the nation – affecting the tax base and the very infrastructure (and security?) of the country.
The metrics for maximizing Public Health includes such things as minimizing death rates, lowering R values.
But how could anyone measure the Public Health misery of the Great Depression?
It is the healthy modern economy in the end that has ensured our long-term high-quality public health, and facilitated our scientific advancements.
All this to say that senior leaders have made and will continue to make tough decisions, some of which may look like they go against the scientific advice of Public Health authorities.
The best decisions are often the least worst, and operational research analysts have crude but effective ways of helping….(identify the problem, identify the metrics by which various decision options can be scored, list the possible actions, list the decision makers and consider the ability of each to make an informed decision, group rank the actions in importance, , etc).
Theirs is not an easy job, and why a given decision was taken may not be the one that any single one of the decision makers would have ranked as #1.
The course of action chosen is not a wrong decision when there is no single right decision available that satisfies all metrics.
Keep up the fine work.
John
Ottawa, Canada
Jaylene writes:
Hi TWIV Family,
I am so glad I was turned on to your podcast. I love the data and topics each show. Even as someone who does not have a degree in science (but has always loved science) it is a very easy to follow show. My husband and I were just listening to your show from Saturday and appreciate the discussion on the opening topic, excessive deaths in people 25-45. Seeing as we are in this age group and have continued to remain vigilant in our precautions this is helpful in combating the naysayers. One thought we also had during the discussion is that another factor to take into considerations of this data is that the number one cause of death in this age group is unintentional injury and car crashes are a big % of the unintentional injury. Since more people are working from home and limiting travel I would be curious to know if car crash deaths have decreased during this time. So not only did you have increase of expected deaths but a decrease in deaths by the number one killer?
The other aspect to this conversation that has been troubling us and not talked about much (at least by people we follow) is the long term illness people in this age group are going to suffer. Considering much of what we are seeing right now the long term issues are heart, lung and kidney disease. So will this create basically an increase in “geriatric disease” in an otherwise young group of people. Therefore adding burden to our healthcare system long term. Since we already knew the baby boom generation is increasing our healthcare costs and if we have another large generation increasing healthcare costs with long term COVID disease, can we really afford to lose more than usual in our prime working age group? How is this going to long term affect our economy? Especially since there is so much concern over shut downs tanking our economy, how will we be able to recover without a full functioning work force in the future. I know this show is more virology based and not an economic show but I would be curious if this aspect is being examined on any level?
Thank you again for your show. Looking forward to the next one.
Best,
Jaylene
Gerald writes:
Hi team. Thanks so much for your terrific podcast. It is very helpful.
Like most of the year, it’s pouring down rain here in Portland, Oregon, though some believe we exaggerate that to keep the tourists away.
So I have a mRNA vaccine concern.
If I understand correctly, the mRNA is packaged in lipids that, once injected, get incorporated into cell membranes. The mRNA then gets translated into proteins (spike) that get mounted on the cell surface. The cell either dies or is killed by immune cells and the resulting proteins are used in the normal way to produce a more general immunity. It works well.
However, the initial cell taking up the mRNA is non-selective and, given the shot is into muscle, would seem likely to be muscle cells. So why doesn’t the bolus of lipid/mRNA also produce a local area of “non-self” cells that are killed off or die? And since the bolus is released in one area, why doesn’t this produce, in effect, an abscess?
This would explain why the shot causes a longer sense of soreness and why the second shot is reportedly much worse.
I have to believe that some people will get a local abscesses— probably more so in the 2nd shot due to the more rapid immune response and abrupt die-off in the area the bolus is delivered.
What are possible reasons for second shot giving more side effects?
Is my thinking wrong? I suppose in the trials it was not seen but I’d like someone to verify that.
That being said, I took Moderna last week and, obviously, prefer the risk noted above to that of getting COVID-19.
Thanks,
Jerald Block, MD
Lance writes:
I had a discussion today regarding getting vaccinated for Covid-19 and regarding vaccines in general. My colleague is skeptical of any vaccinations for the reasons below.
1. Hesitancies about vaccines due to the safety of vaccines and the lack of liability of the vaccine manufacturers (deaths and injuries are under reported or not reported at all).
2. People react differently to medicines so any mandatory vaccinations = bad.
3. Padded statistics: over reporting of Covid-19 deaths, e.g., any death that can be related to Covid-19 will be, even if Covid-19 is not the root cause; therefore, the statistics are padded. I guess my colleague is questioning how bad the pandemic really is. Not really sure.
I am curious as to your take on the above issues especially points 1 and 3. I know you are super busy, and I appreciate any attention you give to my query. Apologies if this is a bit random.
Thank you in advance,
Lance
Jacob writes:
Hello,
I’m writing to you from rainy London. My girlfriend, Dorothy, long time listener, says hi.
Given the current rollout of the COVID-19 vaccine around the world, one question came to my mind, that is:
Why we don’t have robots, machines, booths, whatever shape it takes, for automated vaccination?
What’s the complexity of automating it?
We need to make sure it’s a muscle shot but fat could be measured in a myriad of ways. Perhaps we don’t even need to know anything about it, a change in the profile of pressure applied by the needle could tell us we have successfully breached our way through the skin into the muscle as well. Arm could be put in some sort of frame to make sure it cannot move during the procedure and patients could still be monitored by a nurse or a doctor but, just like with shopping, one cashier per four booths instead of 1-on-1 interaction. Obviously that’s not all but a good start.
As far as I was able to see there are many mass vaccination solutions for cows, chickens and even fish so at least we have tested the concept on animals already.
Lack of similar solutions for humans makes me assume that either administration of a vaccine to an actual human is a tad more complex and upgrading safety of this whole concept to meet required levels is just too expensive (but given what Covid does to economy, is it?) or there are some legal liability reasons standing in the way.
So is there anything in particular from your experience that would explain why we haven’t automated already that seemingly simple aspect?
Cheers,
Jacob
Maureen writes:
Once one receives shot one and shot two is it reasonable to conclude efficacy of the Moderna or Pfizer vaccines would be reached in about 36 hours after the second shot so one is considered likely protected from severe Covid 19 illness from Coronavirus when exposed?
Thank you,
Mo
Juneau, Alaska
Biting icy blustery rain 35 degrees plus wind chill to 28 degrees F.
Maureen Longworth, MD
Retired Physician
Mona writes:
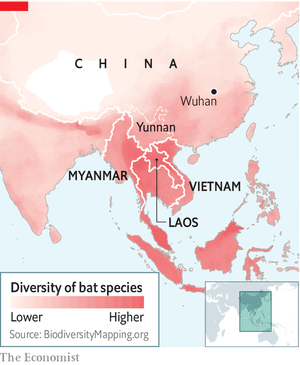
Non-Chinese bats
FYI
The map is telling.
Mona
MAP IS BELOW. Yunnan, one of China’s southernmost provinces, has drawn the attention of virus hunters, as the closest-known relatives of sars-cov-2 are found there. But some think the origins of the virus are not to be found in China at all, but rather just across the border in Myanmar, Laos or Vietnam.
This is the hunch of Peter Daszak, head of EcoHealth Alliance, an organisation which researches animals that harbour diseases that move into people. …. Dr Daszak says that around 16,000 bats have been sampled and around 100 new sars-like viruses discovered. In particular, some bats found in China are now known to harbour coronaviruses that seem pre-adapted to infect people. The chiropteran hosts of these viruses have versions of a protein called ace2 that closely resemble the equivalent in people. This molecule is used by sars-like viruses as a point of entry into a cell. … That such virological diversity has so far been found only in China is because few people have looked at bats in countries on the other side of the border.
John writes:
Dear Dr. Racaniello et al:
Two things, the first of which I guess comes under the broad heading of housekeeping:
I much prefer when there are either four or six of you. Why? Each screen box is the same size. When they’re different, as when there are five of you, there’s a subliminal sense of having two in First Class and the others in steerage. When that happens, is there any possibility of inserting a dummy window so all are the same size?
And then two scientific queries re: vaccine production. Do we have any idea how many doses are produced per batch, and how many batches are simultaneously in production with Pfizer and Moderna / how long it takes to produce each batch?
More importantly – and this could be good ammo vs. anti-vaxxers – what sorts of quality control process applies to each batch? I dipped my toe into this via Google, and only came up with issues of sterile practices. That’s OK but not what I’m interested in.
How is it ascertained that each batch contains what it is supposed to contain, esp since we are in new waters with RNA vaccines? Are for instance cells perhaps transfected with a dose and then examined, perhaps via mass spec, to determine that a protein of the correct molecular weight has been produced? A step even further could be production of a peptide map from the spike to make sure that peptides of the expected molecular weights had been produced, but that would require isolation of the spike first and so might really slow things down. From what I remember hearing long ago in re. production of a peptide hormone, the FDA does not have specific protocols – they rely instead on the producer to suggest appropriate QC protocols, and then approve or deny those.
Finally, I gather that the Pfizer and Moderna RNAs are the same, encoding the 2x proline-substituted Spike protein. But Pfizer’s requires the ultra-cold storage which I presume is due to a difference in the lipid envelope. If that is correct, and since I gather that the ultra-low storage is a significant bottleneck, rather than nattering over whether to give everyone just the first shot, wouldn’t it be better to figure a way for Pfizer to use Moderna’s lipid formulation, free of licensing fees?
With continued admiration for your tireless efforts,
John
Braddock PA – a high here today of 4C, mostly overcast with occasional sunlight flirtations.