
Mary writes:
Dear TWiV Team,
Thank you so much for all you do – I would not be making it through this without you! I have not missed a podcast since my dear friend Neva (from Buda) turned me on to Rich Condit and TWiV back in March.
This week (TWiV 660) during the letters I heard a criticism of Dr. Christian Drosten’s dismissal of the value of rapid saliva testing. Because I’m a regular follower of the podcast, I too caught that, and was at first surprised. So I replayed it a couple of times. What I gathered after replaying is that Drosten’s very sincere observation (apparently contradicting Michael Mina’s input from TWiV 640) appears to be made from the perspective of someone who is not an epidemiologist or focused on public health policy. As Drosten said, he is a clinical virologist. Diagnostics is his métier. And a diagnostician would wish for the very most accurate test. But that is not what Michael Mina was after.
It has been frustrating to me for a long time to hear this type of apparent conflation and disagreement, articulated here by Vincent in his support for the criticism of Dr. Drosten on this point. I think the conflation needs to be dispelled, and I have an idea I have been thinking about.
It appears to me that there are two reasons for testing. The distinction between the two is huge, in my opinion. 1. Diagnosis for the purpose of treatment of an individual. 2. Indication of infection/potential transmissibility in individuals for the purpose of public policy. But people don’t know that there are two distinct purposes.
I’m betting that the first purpose is hugely important in every single person’s mind on account of the scariness of this NOVEL coronavirus. It sort of obliterates everything else. Am I infected? Will I get horribly sick and possibly die? Who does not want to know the answer to this question to the highest degree of accuracy? And, I only want to know it once!
But this highly accurate answer is completely irrelevant to a school superintendent, who has to decide how his school district is going to operate this year, or to a corporate manager who has to decide how his company is going to operate, or to a governor who has to decide what closures to set or lift. The second purpose is vastly more important to our society and to the world. But it is so hard for people to wrap their minds around when they are naturally obsessed with the first.
I think that TWiV can serve a valuable public service in the weeks/months ahead if you guys can clarify the very different purposes of testing. Vincent was right to join in the criticism of Drosten’s dismissive reaction to rapid vs. accurate testing. But the criticism assumes Drosten knew which question he was answering. I don’t think he did.
Warm regards,
Mary
PS: My years working for a federal agency lead me to squirm at the criticisms of the federal agencies charged with administration of the response to COVID-19. There is no ‘them’. There are hundreds or even thousands of individual public employees who have the best interests of the public they serve at heart, for the most part. Some public appointees who may not share that ethic have more power at certain agencies than they do at others. –M.
Jamie writes:
Hi TWiV crew!
I got sick in March, before much was known about SARS Co-V2, and Covid.
Well… other than a certain someone who had by then been told that this thing was deadlier than the flu, but “didn’t want to panic anyone”
( See what I did, Vincent? Didn’t get political at all! )
I knew that I was sick, and I looked for information. Found you guys, and you became my new friends. I laughed at your banter, and absorbed the info like a sponge. It tied me to the world that I couldn’t experience for 91 days.
So… some poetry
A haiku:
Couldn’t leave the bed.
I coughed, alone and so scared.
TWiV was my lifeline.
And a free-form poem
Masks are cool
Just wear one, don’t be a fool.
Before you speak of your rights
Just remember those who lost their fights.
Those who wake up drenched in sweat
From days of torture they can’t forget
They found forms to write their wills
In case they succumbed to all their ills.
Cried out for someone to be there
When they walked too far and gasped for air.
For those who qualify for financial benefits if infected
But false negative tests left them rejected.
For long hauler patients
Who long ago ran out of patience
Whose doctors denied that something was wrong
And they tired of hearing that same song.
Please wear the mask
It’s not just for me that I ask.
It’s for others not yet left with lasting ick
From a virus… the kind that can make you sick.
Anonymous writes:
Dear podcasters,
In today’s episode #661 with Ralph Baric and in the recent episode with Christian Drosten, you asked them what went wrong in the US. Rich also asked Prof. Baric about a “middle way”, that would allow the US to manage the pandemic without the economy going “completely belly up”.
That’s when I thought I would provide you with a different view on the matter and in the process relay my impression on another thing that went right in Germany, adding to the factors Prof. Drosten mentioned (Merkel, early testing).
In May 2020, Easter holidays and Labour Day were over in Germany, the “mild lockdown” was gradually lifted and the anticipated spike in case numbers failed to appear. This left everyone discussing how that could be and how to proceed and which value of the reproduction number to aim for.
Most assumed it would have to be a tradeoff between the economy and public health; aiming for Rt < 1 would benefit public health and be the prudent thing to do epidemiologically, but be detrimental to the economy. Many expected conflicts between social and employer-friendly partys and organisations.
(The idea of reaching herd immunity was already shot down at that point by two statements of the National Academy of Sciences “Leopoldina”, the director of the Robert Koch Institute, Lothar Wieler, and with the help of Christian Drosten and other science communicators like Mai Thi Nguyen-Kim [1] in April)
In this situation, on May 13th 2020, the IFO institute (an independent economics institute associated with the University of Munich) and the Helmholtz Center for Infectiology came up with a conjoint study [2] that was widely spread in all news outlets after Christian Drosten devoted an episode [3] of his podcast to it.
Unfortunately it is only available in German, but its main message can be easily explained using graph #3 on page 5. It shows modeled statistical projections of the monthly economic performance of Germany on the Y axis in relation to time on the X axis and five assumptions of the reproduction number Rt:
– counterfactual (“the epidemic doesn’t exist”),
– Rt=1.0
– Rt=0.75,
– Rt=0.5 and
– Rt=0.1.
The graphs show that it would be ideal for the economy to aim for an Rt = 0.75, as that would allow the economy and society to gradually recover while keeping the initial recession relatively flat.
What the media and science communicators made of this was the message: “Fight Corona or strengthen the economy? Both!” [4] and “Rt=0.75 is the ideal value”.
I believe that from this point on, the whole of society assumed this would be the new goal after “flatten the curve”, acted accordingly and greatly benefited from doing so. Many people then started to gaze at the numbers like deer stare at headlights and what came of that is a different story.
While this study was tailored to Germany and of course there were many assumptions and caveats (many of which are spelled out in the paper), it generally proved to be very useful to be thinking about the management of the pandemic not as “public health vs. the economy”, but to instead realize that both would benefit from doing the right thing. Although now I believe it probably is other people than you who do not get this.
Thanks anyway for listening to my storytelling from across the pond and please keep up your work that I really enjoy watching or listening to.
Best wishes at 414.38 ppm from Freiburg/Germany, where there are 127 µg/m³ CO2 in the air right now.
Armin
PS: I also want to take this opportunity to thank Prof. Racaniello for making his virology course publicly available. I’m currently at lecture #8 but it now takes me more than 8 hours to work through each lecture and I fear I soon won’t be having enough time to follow it further. Keeping up with all the new vocabulary is a real challenge, but I expect to become more fun at parties the longer I keep it up.
PPS: I hope y’all know about https://deepl.com, which is a machine translation website whose results are far superior to translate.google.com in many cases.
Footnotes:
[1] Dr. Nguyen-Kim’s comment in Germany’s daily most watched (by far) TV show: https://www.youtube.com/watch?v=N8R_p-awmgI (you can let the subtitles be automatically translated, it’s not perfect but you’ll get the message. “Mr. Immunity” means herd immunity (German word Herdenimmunität gets misinterpreted))
Her youtube channel: https://www.youtube.com/channel/UCyHDQ5C6z1NDmJ4g6SerW8g
[2] https://www.ifo.de/DocDL/sd-2020-digital-06-ifo-helmholtz-wirtschaft-gesundheit-corona_1.pdf
(in German)
[3] Das Coronavirus-Update, Episode 41:
https://www.ndr.de/nachrichten/info/coronaskript196.pdf
[4] https://blogs.faz.net/fazit/2020/05/15/corona-bekaempfen-oder-wirtschaft-staerken-beides-11383/
Justin writes:
Emails offer look into whistleblower charges of cronyism behind potential COVID-19 drug
Richard writes:
— Vincent et al on the TWiV team.
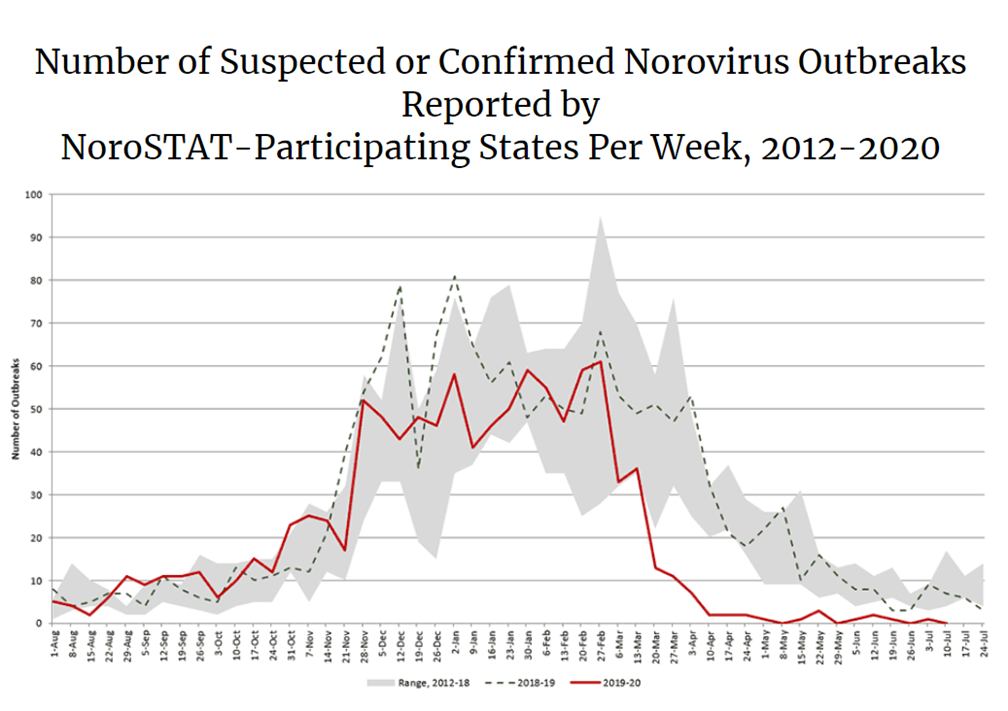
I am a general surgeon at Houston Methodist Hospital and recently presented a case of a patient who thrombosed her superior mesenteric artery after a Norovirus infection diagnosed on GI Panel PCR. In my research for the presentation I came upon the CDC website which showed this graph of Norovirus outbreaks since 2012. Since March 2020 it is much less common to have outbreaks. With less food handlers in restaurants, cruising at a standstill, largely absent team sports, social gatherings significantly decreased and new compulsive handwashing, might we not also expect a decrease in the incidence of seasonal flu, rather than the dire predictions of a combined pandemic and the flu season??
Love the show, it lengthens the time my dog gets to walk.
I am Learning and laughing.
Richard E. Caplan, MD, FACS
Houston Methodist Hospital
Houston Texas
Pamela writes:
Today in the NYT there was an article on the possibility of developing some immunity to covid19 by mask wearing. Because you may get tiny doses of the virus through the mask but not enough to make you sick, you become asymptomatic and then immune. I think they called it variolation or something like that. Could you discuss this?
Thanks,
Pam
A study published in May by scientists at Public Health England’s National Infection Service at Porton Down, Salisbury, gave ferrets varying doses of Sars-Cov-2 and found a clear difference in outcomes.
As the geneticist and epidemiologist, Francois Balloux points out: “There are loads of examples in the literature for symptom severity being dose-dependent for plenty of [other] bugs.” The most obvious is the flu. A major 2010 study of influenza A concluded that there was a clear relationship between the infectious dose of that virus and patient outcomes.
Ken writes:
Hi Twiv!
Greetings from southern Marin County, CA, where the outside temperature is currently 73 degrees F, the air quality is currently 112 EPA PM2.5 (purpleair.com; sensor outside my home), and the sky color is currently — what would you call it? — apricot?

Photo: 9/9/20 11:50 AM
First I have to say: TWIV is the best. Who knew that a podcast about virology could be so entertaining and somehow reassuring and comforting to listen to, in addition to informative? It is all those things and more. Thank you!
Like a lot of people on the west coast right now, we are feeling like we gotta get out of the place. We are thinking: East Coast. Our question to you: Fly or drive? Which is lower risk in your estimation? Assume all normal, TWIV-endorsed, regular-person precautions are in place, and that no camping will be undertaken.
Warmest regards,
Ken
Greg writes:
Hi TWiVers!
Weather in Seattle, WA:
- High of 84 F
- Sunny with a hint of wildfires
- 77 new cases of COVID-19 per 100K over last two weeks (per King county’s excellent dashboard)[1]
Thank you for your work in building a bridge across the MoAT (Miasma of Anti-Think], so that we might defeat the crowned virus in its capsid castle!
Immunity Certificates
I’ve been an avid listener of TWiV since March. I was quite taken by Brianne’s Brianalysis and Alan’s Alambasting of Immunity Passports in TWiV 603.
Interlude haiku
Rac-an-yell on, please!
Testify, TWiV, your beliefs;
The truth must have teeth
Brianne and Alan suggested that the perverse incentive created by immunity passports could cause some folks to intentionally seek infection if doing so gave them greater access to jobs or social opportunities.
But some quite intelligent people have been in favor of some form of immunity passports. As expressed in a JAMA viewpoint by Ezekiel Emanuel, bioethicist at UPenn and NIH, it might be reasonable to require immunity certification for employment at elder care facilities or in other limited, high-risk situations.
Of course, the ideal answer is Mina-style frequent, rapid testing. But if that fails to materialize, and technical issues around correlates of immunity and serology-testing specificity are resolved, it seems plausible to me that the immunity passport debate could resurface (particularly if there are significant delays in developing an effective vaccine).
But what about this perverse incentive issue? Would people actually intentionally seek out infection? When smart people disagree on theory, we look to data!
Professionally, I work with a team of thoughtful and socially-minded software engineers to build an intuitive statistical analysis tool (“Stats iQ“). Our team decided to investigate. We surveyed a representative group of 1000 Americans on whether they would intentionally seek out infection in order to earn an immunity passport.
- 11% of U.S. adults say they would “probably” or “definitely” seek infection if that was required to maintain or access employment at an eldercare facility.
- 13% of U.S. adults would do so just to visit eldercare facilities
- 14% of U.S. adults would do so to go to gatherings greater than 25 people
Those are not all the same people saying “Yes” each time, so in sum more than 1 in 5 Americans would seek out infection for one benefit or another (fuller findings here).
That willingness to seek infection was concentrated in the young (quite predictably) and, for employment-related questions at least, in the economically insecure (quite depressingly). Political leanings were not correlated with this willingness, at least after controlling for other factors.
I was open-minded initially, but I am now quite convinced that immunity passports should not be implemented. Hopefully this research serves as a nail in the coffin of that idea.
If anyone is interested in learning more or in playing around with the data we collected, just search for “stats iq immunity passport study”[2] (here’s the direct link to the results and to the underlying data)
Parting thoughts: Most of us can quickly call to mind the face of a nurse or other medical professional we know. And, for all our society’s flaws, the vast majority of us can intuitively appreciate their contributions in this dark time. But, to many of us, scientists are often faceless, removed, even abstract. Thank you for putting a face on science, for showing us it’s humanity. We’re all in this together.
Greg
[1] Happily, that last figure is dropping pretty linearly by about 17 per month over the past two months. If that trend continues even a tiny bit longer my kindergartner, June, should be in school in person soon!
[2] In case any TWiVers look at the article, I need to defend our terminology! In the survey we used the phrase “the COVID-19 virus”. We worried that some folks would not know the term SARS-CoV-2. We believe it’s reasonable to call it the “COVID-19 virus” (the virus that causes COVID-19) just as one might talk about “flu season” (the season that causes increases in flu).