
Jonas writes:
Dear Vincent, dear Christian,
I was very excited to hear you will renew your dialog from TWiV #601.
I would love to hear you discuss the home testing approach a la Mina, in the differing contexts of the US and Germany. Let me explain:
Christian mentioned in passing in his own podcast (first episode since Mina TWiV due to summer break) that he believes asymptomatic testing makes sense in the US right now, but not in Germany. He also talked at length about antigen tests in the context of contact tracing by health care professionals.
While I believe those are exactly the right next steps, I do feel there could be a role for routine at home testing of asymptomatic people further down the road: rather than self quarantine completely for a week before visiting grandma (as Prof. Drosten proposed), I would rather take 3-4 home tests on consecutive days, to ensure I am unlikely to be infectious.
What do you think about this?
Best regards
Jonas Binding
(founder of rapidtests.de, the German sister site of rapidtests.org, which you have mentioned on TWiV twice before)
Mary writes:
Questions/comments for TWiV with Christian Drosten
I regard Christian Drosten as the foremost world expert on coronavirus, in all its complexity. My one regret is that his writing and podcasts are not widely available in English. Perhaps we would be in a better place now if they were!
1. Origin (and risks of re-introductions). Has there been any progress in investigating possible intermediate hosts, such as raccoon dogs or mink which are intensively farmed in China and other countries? Recent transmission studies have added fur to the list of transmission routes, as a fomite and re-circulated through the air. Might this have any potential relevance to fur farming, as well as livestock and pets, playing a role?
2. Avoiding lockdowns. Your proposed second wave strategy focuses on identifying and controlling clusters rather than cases. What kind of testing would you base this strategy on? Would Michael Mina’s home instrument-free antigen infectivity indicator paper-strip tests be one component? You also propose ‘short’ quarantine/isolation times. Again, would Mina’s proposed 5 days of infectivity, if reliably identified, be compatible with your strategy or do you have something else in mind?
3. Immunity memory. Do you think that loss or reduction of immune memory following natural measles infection may be playing a role in severe or even asymptomatic Covid cases, especially in children (and anti-vaxxer families)?
4. Surprises and long haul complications. The consensus seems to be that Covid-19 is full of surprises, mostly nasty ones, that we are finding almost on a daily basis. Is this because of the uniqueness of the virus or because we are investigating with unique intensity? Or, as we are beginning to find with Zika, Dengue and Ebola, will there be nasty surprises with other EIDs if we look hard enough?
With many thanks to all of you!
Mary
EID Policy Researcher
Kyle writes:
Hi TWIV,
I am American in Germany who has been listening to you since March and have gotten a lot out of your insights. I work with data but not in a scientific context, so it’s been nice to have someone provide a bit of context to all the numbers we see flying around.
I thought it might be interesting for you to see some of the highly detailed data from Germany in preparation for your follow-up podcast with Christian Drosten.
The Robert Koch institute (German CDC equivalent) publishes daily briefings on the outbreak, with some weekdays dedicated to more detailed topics. Out of these, I think the Tuesday and Wednesday reports are the most interesting, so I will excerpt and share a couple details.
You can see the archives here: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Situationsberichte/Archiv_August.html
Last week’s Tuesday report here: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Situationsberichte/2020-08-25-en.pdf?__blob=publicationFile
And the Wednesday report here: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Situationsberichte/2020-08-26-en.pdf?__blob=publicationFile
To me, the most interesting of this data is the cohort analysis, showing the hospitalization and case fatality rates by people infected per calendar week (Tuesday, page 6):
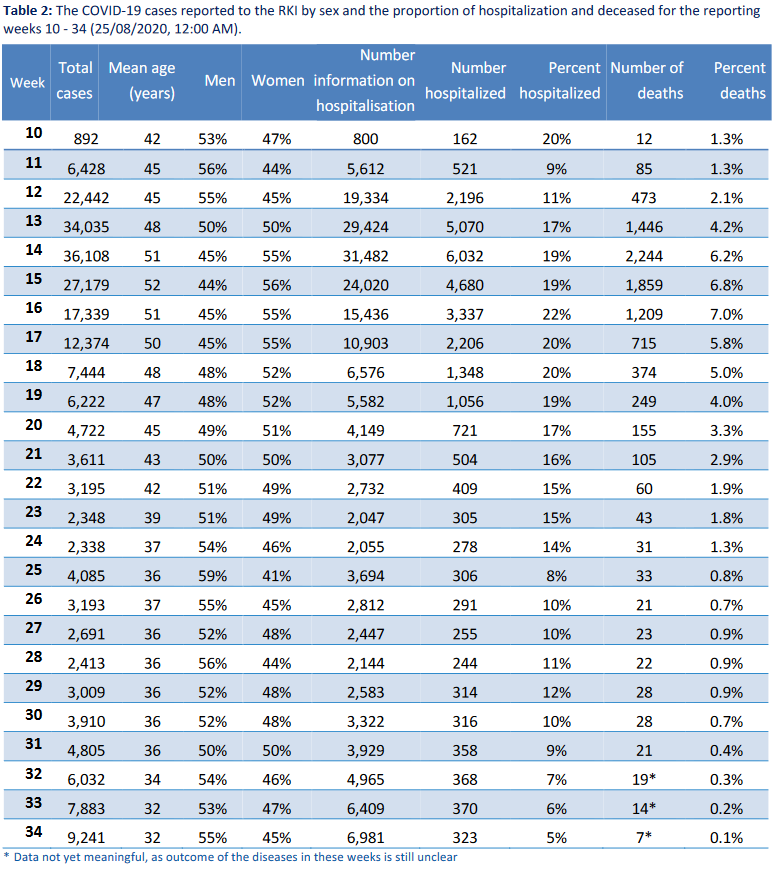
From this, we can see a fairly steady drop in CFR down to less than 0.5% in the most recent weeks with settled outcomes. There seem to be a couple data points in the table and others that are quite correlated to the reduced CFR, although I would be interested to hear someone (maybe like Dr. Drosten) expound on the weights, to the extent speculation is already warranted.
I know this question of declining CFRs is on the tip of many people’s tongues, and I think that Germany is starting to provide the kind of data that could even be modeled, potentially.
What we can see right away:
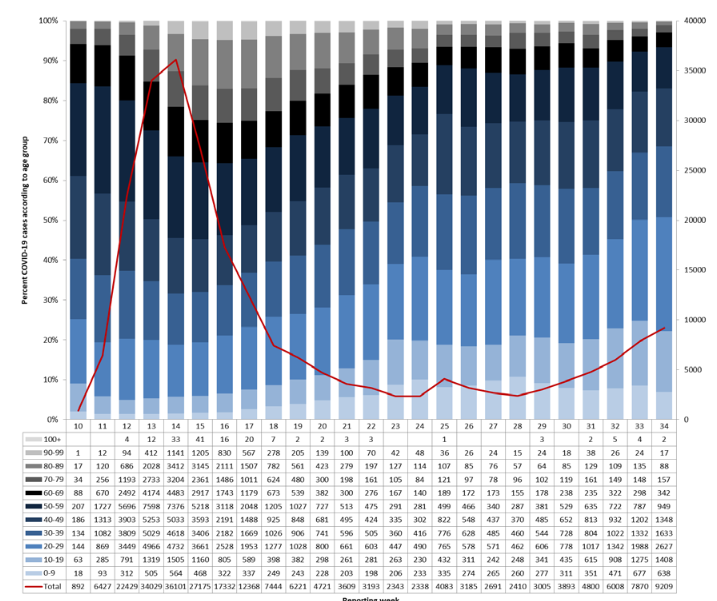
1. Average age is dropping – but this is likely made up of a couple of components:
– Better testing and tracing catching less severe cases, meaning that we’re catching younger people. This may mean that the average infection age may not have dropped much, but the average case age has dropped a lot.
– That older people and older person care facilities are being more cautious (this is anecdotally observable in daily life in Germany), meaning the average infection age has in fact dropped.
I don’t know what share of reduced average age is just observation and what part is real.
We have a really nice and detailed chart showing the age distribution of cases over time in the same report – revealing that many fewer elderly infections are occurring – now down to around 30 per week over 90 years old from well over 1,000 per week before. (Tuesday, Page 5)
2. Positivity Rate, shown in the Wednesday reports are also dropping and are steadily below 1% now. This lends credence to the idea of catching low severity cases (Wednesday, Page 9):
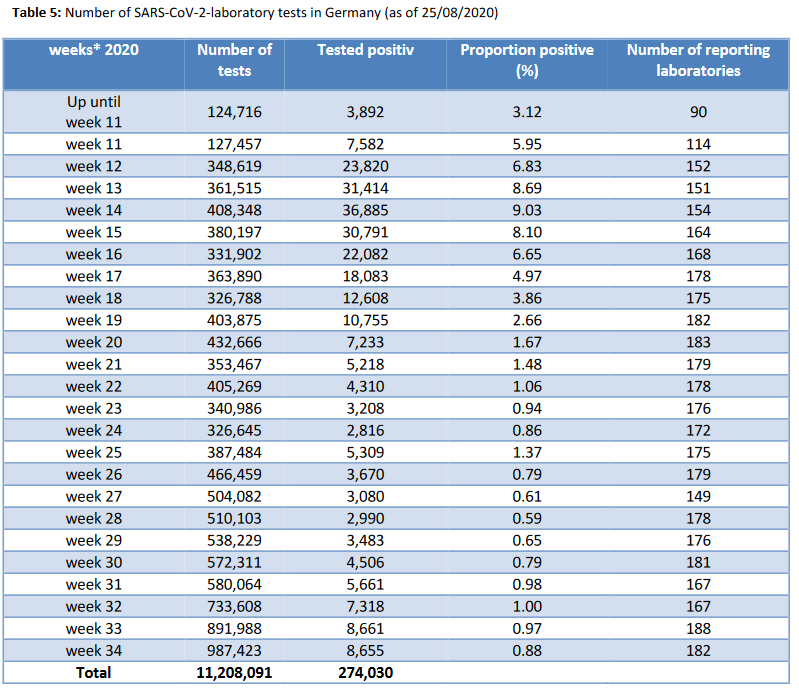
3. It is also interesting that the most recent drop in CFR is quite closely linked with the starting of testing of travelers arriving from high-risk regions. I don’t know if this is because they are catching more low severity cases by testing regardless of symptoms, if they are sampling from a younger population, or if this is just coincidental to the reduced fatality rate.
The authors do note in the Wednesday report that the positive rate at the borders are around the same level as the general testing positivity rate. So there is clearly a quite high risk associated with travel. (Note, I don’t know how to reconcile there being mandatory border testing from high risk areas turning up 600 cases with the below reported 4,000 cases from abroad, most of which are from the same few countries). Excerpt from Wednesday page 9:
In the Tuesday report, we also see very good data on the probable location of infection over time. The authors note that 1/3 of cases do not have origin reports, meaning that the share of foreign exposures must be something like 50% of the total. The chart below uses all cases as the denominator, whether they know the origin or not. (Tuesday, Page 8)
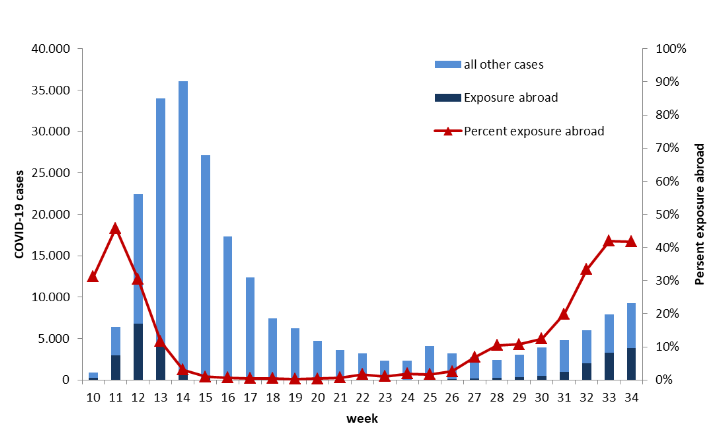
This shows that the number of domestic transmissions has been relatively flat and that the recent surge appears to come from importation. Although there was a period in July where the borders were open but there was no mandatory testing for arrivals where the numbers may be misstated.
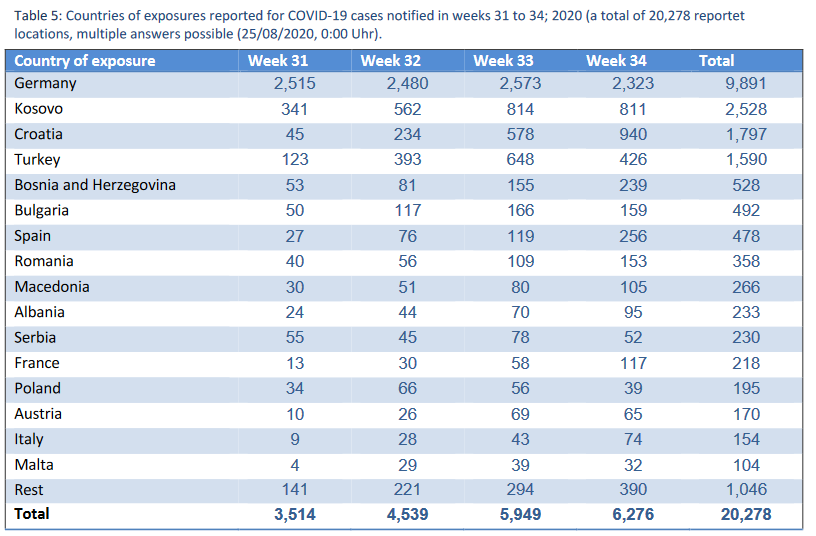
They also provide a report of origin by country for the known cases. Here you can see that out of the known origins, the majority are coming from abroad and reported domestic transmissions have actually dropped slightly (though maybe due to missing data) across the last month. (Tuesday, Page 9)
Anyways, whether or not this spurs any specific questions for Dr. Drosten, I thought it would all be quite nice reading in general, but especially in prep for your discussions on “das Coronavirus!”
A rhetorical question I will ponder just while I am here: The only thing that the Trump administration can claim as a relative success is a moderate CFR. Now there are discussions of reducing testing on pre / asymptomatic cases. Aside from the human consequences that reduced testing likely causing increased spread and misery, isn’t it bad politics to pursue a policy that deflates your one assertion of competence?
Regards from Germany,
Kyle
Dave writes:
I think you buried the lede when discussing Fauci’s podcast appearances:
Whether by design or not, Dr. Fauci has effectively circumvented efforts by the White House to mute him. Since Mark Meadows took over as chief of staff on March 31, White House communications officials have approved very few requests from major outlets. But there is no such review process for smaller ones, like the weekly podcast of the Journal of the American Medical Association, or the KC O’Dea radio show.
It seems likely that Fauci’s podcast appearances were because he was muzzled by the current administration from appearing on TV. They forgot to explicitly forbid podcasts and alternative venues and Fauci dutifully tried to get his message out via these alternative mechanisms since he needs to contradict the falsehoods coming from elsewhere (e.g. CDC, FDA).
Regards,
Dave in Oakland (72F)
Aileen writes:
Good morning!
It is a sticky 82 degrees in Holland, PA. My husband introduced me to your podcasts about a month ago and I have been listening to them almost every day since. Thank you for being a source of unbiased scientific information in such an uncertain time.
I am writing today because many schools in my area are reopening and their instructions for parents state that no backpacks or reusable containers are allowed in the classrooms. This means all children must bring disposable lunch bags and drinks.
This confused me since I thought that most transmission happens through droplets in the air. I thought that there wasn’t much concern over surface transmission. Also, with the “distancing” in the classroom, the lunch containers would only really be touched by the owner and maybe the teacher.
Is this precaution necessary? It seems more harmful to the environment than beneficial to anyone’s health. Am I missing something?
Thank you for sharing your knowledge with us all!
Aileen
Bucks County, PA
Caryl writes:
Please help me make some sense out of this story from Kaiser Health News:
Does this make any sense? What about the 40% who don’t have symptoms?
How different are these tests from the rapid testing supported by Michael Mina et al?
Thank you for all you do. TWIV is my most trusted news source.
The interview with Robert Fullilove was amazing. So much of the news is framed in pessimism these days; his optimism is inspiring.
Caryl, an RN
Charles writes:
Hello TWiVers;
Just a pissed off human living in Chapel Hill where the weather is OK at 81F (27C) with a bit of rain.
Convalescent plasma, “truly historic announcement”, yea right. “We dream in drug development of something like a 35% mortality reduction,” is just BS. No control, no possible measurement of mortality reduction. Oh, more BS about the 35%, to me a 35% reduction in mortality at this point in time means that of 100 sick people that would have died, now only 65 will die. That does not seem to be what Trump and Azar mean. See the stat news article or In The Pipeline.
Fatalities from COVID-19 that I will really miss:
1) John Prine, singer and songwriter.
2) Trust in the CDC as expressed by Alan Dove in a late May 2020 TWiV: “We have indeed come to a point where we do have to second guess announcements made by the CDC.”
3) Trust in the FDA. As shown by their inability to see the light of testing for the infectious and their BS from Sunday.
Thanks for letting me vent and on a positive note, for the work that has gone into TWiV,
P. L. Charle
Elise writes:
Hi TWIV friends- I am a pathologist from New Orleans, LA.
I love your show!
A limerick I wrote for you…
There once was a Dr. called Fauci.
He deems America’s Covid response quite slouchy.
He advocates isolation and testing is the rule
While implying that Trump is a fool.
This makes our ‘emperor’ quite grouchy.
Elise MD
Verlon writes:
Greetings TWIV,
I’ll start with the usual comments:
· Love your podcast and the serious, rational and scientific discussions about COVID-19-related and other infectious disease issues. (Given our long connections with Liberia, Ebola was of special concern.)
· As many listeners write, I only really understand about 1/3 to ½ of the detail, but get the main points and the issues, a very valuable information and educational service.
· I’m not a “hard” scientist nor an academic. (My decision to change to the arts and humanities was based on my love for its subject-matter, but was finalized at the time I set the record for glass breakage due to an explosion in my undergraduate organic chemistry lab, a record I’m told held for at least 50 years.)
From multiple TWiV discussions, I know some of your panelists/guests love participating in musical performance activities and are as anxious as our choir is to resume rehearsals and performances as soon as possible, but in a manner safe for the performers and the audience (congregation in our case). On TWiV you’ve discussed and evaluated a number of schemes to enable resumption of rehearsals and performances, but I don’t think you’ve yet judged any approach to be safe, especially for choral performance.
The latest scheme circulating among our choir’s e-mailing list is a “Singer’s Mask” supposedly “developed by singers FOR singers by Broadway professionals to help contain droplets while allowing space around the mouth to sing comfortably” (https://www.broadwayreliefproject.com/). Sold by the Broadway Relief Project and presumably for a worthy cause, I’m skeptical that it can actually work effectively, especially for professional singers with well-developed techniques to empty their lungs of air, sound and droplets.
Your professional opinion(s)?
Hope my qualms are judged wrong by the TWiV gang,
Verlon Stone, Ph.D.
Special Advisor, Indiana University Liberian Collections/African Studies Collection
IU Libraries
Research Associate
Folklore & Ethnomusicology Department
Anonymous writes:
Hi all,
I am just a med student at Stanford (and very long time listener, you all helped prompt me to pursue medicine years ago). Given all the talk about reopening schools, I thought you would be interested in Stanford’s approach.
They never were willing to do frequent testing, their requirement is to do two tests a few days apart after arriving on campus, and then monitor yourself for symptoms and report them daily via a cumbersome website that encourages copy/paste. Originally they were going to have undergrads come back on campus in staggered groups, but now they are doing most of undergrad online, which is great since their testing plan isn’t exactly ideal.
However, grad students and a fair percentage of undergrads are going to be back on campus. You would think they would do frequent testing and implement sensible processes for this small number, but no. Instead they have created a ‘campus compact’ that all students have to agree to to be enrolled. It authorizes the school to use a vaguely defined compact review board to investigate any breaches of compliance with their policies and impose almost any sanctions including kicking students off campus. Their policies aren’t necessarily terrible, but they are draconian and frankly weird. I doubt students will be able to comply with them completely, and even if they do we will have no idea if it is working because they won’t do any testing. Plus they are still doing in-person exams and having students share a house (with a requirement to physically distance from your housemate, as if this will stop transmission).
I personally feel like this is the school shirking responsibility for testing and trying to put all of the responsibility on students by essentially saying that if they don’t follow all policies perfectly, they could be aggressively punished by a shadowy review board.
Thanks, and please keep me anonymous for this one.
Judy writes:
Hello TWIV gang!
I’m me again. I remain a loyal listener but from the sounds of it, you have gained many more since my first email to you on February 10th. My, how much has changed! The weather, however, remains around 30C in Singapore. Being close to the equator, there really isn’t much difference between February and August.
I don’t have a limerick or haiku but I do have a question. Being in Asia, I often talk to my colleagues in mainland China and for a few months now they have been telling me that the Chinese media thinks the source of infection in areas that had been virus free for many weeks comes from imported Frozen Food, specifically from S. America where there have been uncontrolled outbreaks.
I kept looking for similar reports in Western media, but what little I could find theorized it was highly unlikely, but I could not find any actual published experiments. It wasn’t until the fresh outbreak in New Zealand did this theory come into prominence in Western news.
And then yesterday, I saw this article in Forbes that refers to the below link from BioRXIV (preprint)
https://www.biorxiv.org/content/10.1101/2020.08.17.255166v1
What does the TWIV team think about this? And what are the implications of this to all of us buying frozen meat and seafood at our local grocery store? Should we be concerned?
Regards,
Judy
PS. I said “Infectious” not “Live.” The TWIV team has trained me very well.
Amy writes:
Hi TWiVers,
I wonder if the team has ideas or perhaps Daniel Griffin could help with this question.
You hear a lot about how the 1918 flu had a high mortality rate in young people because they experienced cytokine storms. The explanation you hear is that they had well-functioning immune systems and that made them prone to the immune system overreaction.
Now we are hearing how COVID-19 severe illness and mortality is linked to whether infected people experience a cytokine storm. But now the people most at risk of dying are older.
How do we put these two examples together and make sense of them? A friend of mine wondered if the cytokine storm associated with COVID-19 might be connected to some earlier infection in their lives. Could this be the case? It might explain why older people are more likely to react badly to SARS CoV-2.
What do we understand about the risk factors for a cytokine storm for a COVID infection? And does this new virus change the way we understand mortality risks of the 1918 flu?
Thank you! I can’t tell you how much I appreciate your podcast and how often I recommend it.
Amy
Portland, OR
Richard writes:
Hello twivercites,
Firstly its 19C° and Sunny here in Melbourne Australia with a so called second wave (I think its a second peak of the first.) Of SarsCoV2. I am just a paramedic and as such I do often come face to face, via an N95 mask, with this virus. This has caused anxiety in my 7 and 8 year old kids. I try to make videos for them of my work and how we employ processes to attempt to mitigate our exposure to risk.
Tonight my youngest asked me what happens to a germ’s body after it dies. I explained a bit (partially guessed) about bacteria decomposition and being re-used by other organisms including us. He then asked about viruses. I said that viruses aren’t alive. He disputed this by explaining that Corona viruses are happy and that if viruses can be happy then they must be alive. I love this definition however I feel it may be hard to come up with an experiment to prove or disprove it. He proceeded to explain that influenza, ebola and Ross-River all looked happy but herpes, chicken pox and polio all seemed sad. Perhaps he can be a new diagnostic tool? Anyway he finished by telling me that I should let “that yelling guy” (Vincent) know and he would prove that my son is correct. So I am.
Secondly one of my colleagues is bee keeper. (I am also but I only have 3 hives so not a real one.) He is worried about catching covid from his bees. I pointed out that most people are very good at physical distancing from bees so he should bee fine. It did make me wonder though is Sarscov2 able to infect insects? Are any Coronaviruses? I’d love to hear your thoughts on this.
Thanks for all you do, its educating myself and many other ambos (paramedics) in Australia.
Stay Grumpy Vincent.
Richard
Agda writes:
Hello Vincent and team,
greetings from chilly Berlin (15ºC)! Everybody is talking about Sars-CoV-2 reinfection these days, the latest report includes multiple tests, serology, and specific testing for sample mix-up/contamination – going even further than the HKU paper (https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3681489).
At the same time, Shane Crotty (and I’m sure Christian Drosten will say the same) is convinced that very few people won’t seroconvert at all. Which is reassuring; however, does it answer all the questions about the infection/reinfection kinetics? Can we confidently say that reinfections are very rare exceptions to the rule? It would be great to hear from Jon Yewdell on the open questions about respiratory viruses reinfections or from Marion Koopman (who’s been involved in researching reinfections in the Netherlands, among many many other things).
Thanks a lot for all you do,
Agda
Nancy writes:
Hi TWiV-after the last episode, I thought about this article and book for Vincent (And everyone!). I don’t know if I agree with all of his conclusions and there may be other good books on the subject, but this guy has been thinking about some of the problems Vincent is concerned about for a while. At the least, the history and psychology are interesting. The pandemic surfaces how absurd people have become about their ‘belief’ in science but it’s a real problem for all of us. (I believe the title says it all!)
The Death of Expertise: The Campaign against Established Knowledge and Why it Matters
There is a shorter article he wrote as well
https://thefederalist.com/2014/01/17/the-death-of-expertise/
LOVE the show!!
Nancy