
Susan Weiss writes:
I really enjoyed TWIV today. I have a couple of comments about topics discussed.
Persistent CoV RNA. A big question for MHV, around for many years, is how does MHV RNA persist in the CNS, probably for the lifetime of the mouse, long after infectious virus is cleared. MHV causes acute encephalitis followed by chronic demyelinating disease (MS model) and while virus is cleared by about 10 days pi, viral RNA, both genome and mRNA can be detected for months in the brain and spinal cord (papers from our lab, Conni Bergmann, Susan Baker). Given that there is RNA and mRNAs, we tried very hard to recover infectious virus initially by immune suppression and later by making brains lysate from mice with persistent RNA and inoculating into the brains of naive mice, a very sensitive assay and no transmission of virus. The viral RNA persistence remains unexplained.
Detecting RNA by PCR. (maybe you have discussed all this; I have not heard every TWIV).
There are some unclear issues, like are the samples for testing (nasal or endotracheal or saliva) containing virus only or infected cells. We could design a test for mRNA specifically by using primers that cross leader-body boundaries but this is probably too much for a rapid test and maybe it wouldn’t least tell us that virus is replicating- as there could be fragments of mRNA as well as genome. But if there were large amounts of mRNA compared to genome it would suggest replication. Also, when genome copies are quantified, it is not clear to me for any given test whether it is genome copies/ul as often expressed or for the entire patient sample which is diluted into the test. We found if we have less than 105 genome copies/ul in a clinical sample, we cannot recover infectious virus. But 105 copies may only represent 100 PFUs (CoVs definitely make a lot of noninfectious particles). And I think we have no idea how many PFUs is an infectious dose for humans. We and others around us have calculated genomes /PFU several times and get varying results. Bottom line is it is difficult to know how many genomes are likely to signify viral shedding.
Susan
Susan R. Weiss
Professor and Vice Chair, Department of Microbiology
Co-Director, Penn Center for Research on Coronaviruses and Other Emerging Pathogens
Perelman School of Medicine
University of Pennsylvania
Bill writes:
I first heard of this last week in a brief news announcement, but as it didn’t include any details or links, I only briefly mentioned it to my sister Kathy. This week CU Boulder put out a more detailed news announcement with a link to the MedRxiv preprint… https://www.colorado.edu/today/2020/07/22/new-covid-19-test-returns-results-45-minutes-without-nasal-swab . The test uses an RT-LAMP assay, and the saliva sample, after adding a buffer, is boiled (?, see comment below) put into 3 different enzyme mixtures, and heated to 65ºC for 10 minutes after which reactions are stopped by heating to 80ºC. If the color changes from pink to yellow, the test is positive.
I don’t fully understand the accuracy discussion…they used 60 “contrived” saliva samples, 30 positive and 30 negative. All of the negative samples evaluated properly, while 29 of the 30 positive samples were evaluated properly, giving what was described as a sensitivity estimate of 97%.
It obviously takes 45 minutes rather than 10 minutes, and it requires several enzyme mixtures which I’d like to think would not be hard to acquire.
As to the “boiling of saliva,” this was done by immersing the saliva tube in a 95ºC water bath for 10 minutes. First, I wonder if the saliva was really boiling, and secondly, I note that Boulder, Colorado is 5,328 feet above sea level, and the nominal boiling point of water at this altitude is 94.65ºC.
—
Bill
*
Erik writes:
I’m writing from Portland, Oregon (currently 68F and clear, at 1am PST). I’m a sculptor and graphic designer, and I keep hearing “Countering a miasma of anti-think” in my head, which seems to pair nicely with what I’ve been saying too often these days: “we’re drowning in an ocean of stupidity.”
Anyway, I figured I’d take a stab at designing a shirt featuring the famous line. Images are attached, as well as print files if you’re into that sort of thing.
I really enjoy the podcast and recommend it to all of my friends, thanks for all you do.
—
Erik

Kyle writes:
Huge fan of the show! I actually came across the show through Dr. Vincent Racaniello by way of his lecture on macrophage.co. I have been listening to the episodes on COVID-19 (naturally), and I had somewhat of an epiphany. Is it possible that ACE2 is highly conserved across animal taxa, which could explain the success of CoV2 transmission from different animal species, most recently the tiger case? I know there are examples of certain biological molecules that are conserved, so I am curious if this may be such another case. I did a cursory search of the literature, but found no references.
My background is Evolutionary Biology and I teach A&P, and I am definitely planning on incorporating what I am learning about SARS-CoV2 and others in my lecture!
Best,
Kyle
Don writes:
TWiVers,
Fortunately, I did not have to send you a message about Amy Schumer, but I do want to point out that the Jonestown massacre used Flavor Aid not Kool-Aid: https://en.m.wikipedia.org/wiki/Flavor_Aid
I love the show, even though you guys often say “infectious dose”, which is a misnomer… median infectious dose would be better.
– Don
Paul writes:
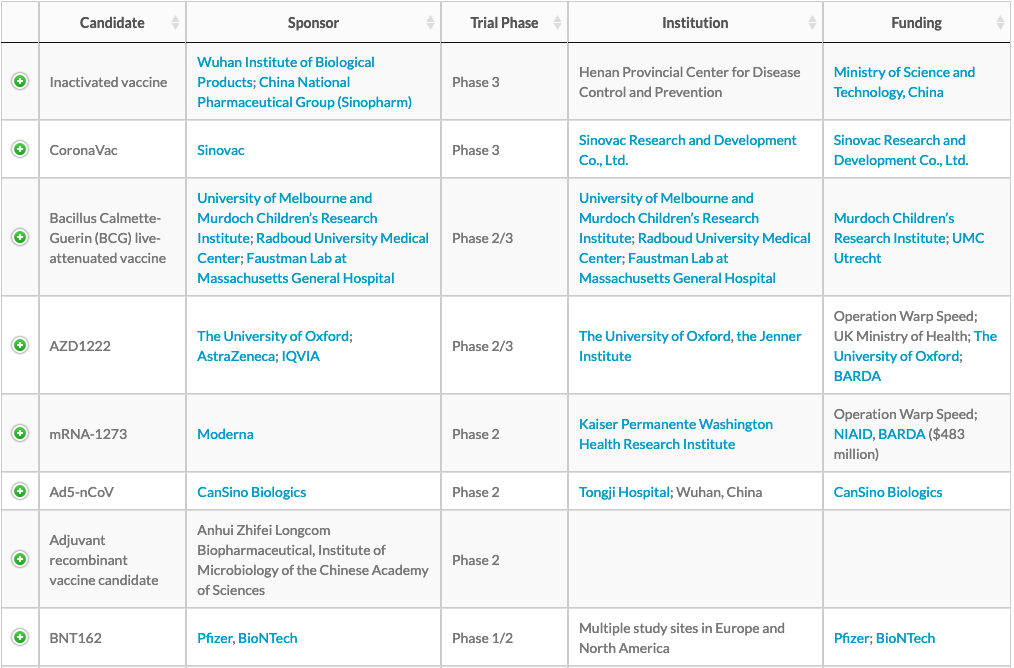
I’ve been hearing a lot of trumpeting today about the Moderna and Pfizer vaccine candidates going to Phase 3 (or 2/3) trials. But until now, I’ve heard mostly about Chinese and Oxford candidates.
This is the RAPS summary of the advanced candidates, as of July 23. Have Moderna and Pfizer jumped to the top of the list? Are they in 3rd (Moderna) and 5th (Pfizer) places? Do Pfizer and Moderna just have better PR machines than the Chinese, the BCG group, and Oxford?
Paul
Lexington, MA
Amy writes:
Hello to the TWIV team,
I am “just” a child psychiatrist who had been turned on to TWIV by my children’s pediatrician whose husband is an infectious disease epidemiologist and after years of anxiety about the next flu pandemic, I called her in mid-january when reading about SARS-CoV-2 and said, “this is it” and she responded, “yes.” When I went to telehealth in early March, my patients thought I was over-reacting, and kept insisting they would see me back in the office in 2-3 weeks, and I corrected them that the 2-3 was correct, but it would be more like years. Despite disliking the way infectious disease was taught in medical school, I find virology and microbiology incredibly interesting and understand that microbes were here long before us and will be here long after we are gone.
I want you to know that one of the only things that helps keep me calm and sane while working full time (from home), taking care of my two small children, supporting my husband who is their primary caregiver and supporting my friends and patients has been your smart, thoughtful, humorous and sophisticated discussions on all things COVID. It calms me to know there are thoughtful people out there metabolizing all this data and thinking deeply about not only the virus but the implications of our policies and our practices. My good friends call it my “COVID porn.”
Thank you from the bottom of my heart for the work you do. I will continue to be a supportive listener and am so grateful for this podcast. I know you’re working hard, and it is much appreciated.
Stay well!
Amy
David writes:
Hi Vincent,
On TWIV 648 an email asked if the kind of rapid testing that Mike Mina is advocating has been tested in a community trial. The Gates Foundation is sponsoring just such a trial, SCAN. The work was halted by the FDA in May (https://www.nytimes.com/2020/05/15/us/coronavirus-testing-seattle-bill-gates.html) but has since restarted (https://publichealthinsider.com/2020/06/10/greater-seattle-coronavirus-assessment-network-scan-resumes-covid-19-testing/). Here is a link to the preliminary results prior to halting of the trial https://publichealthinsider.com/wp-content/uploads/2020/06/new-technical-report.pdf An important finding, 87% of respondents with a positive result had not sought in-person clinical care before enrolling in SCAN so at home rapid testing does quickly identify many new cases of COVID-19.
Keep up the great work,
David
P.S. Full disclosure, my company is developing COVID-19 diagnostics, but we are not involved with the SCAN study.
David J States MD PhD FACMI
Chief Science Officer
Angstrom Bio
Austin, Texas
Jackie writes:
Dear Vincent and TWiV team,
I am writing you from Burlington Ontario, Canada, where it is 19C or 66 F. I started listening to the podcast after Malcom Gladwell first recommended it in early April and I have been an avid listener since.
My husband and I are just humble musicians, he plays the trombone and I play the saxophone. We perform with groups that range in size from a quartet to full orchestra. As you are aware, our industry has been completely shut down and it appears that it will be for some time to come. This has been challenging on a few levels but it has been especially difficult socially as playing music with other people is part of what keeps us sane.
I am truly grateful to have found your podcast and I am learning so much. I admire you all because you still have an awe inspiring zest for learning. Music and science are very similar in that you are never done learning new things about them. I have always told my students that music is infinite. So too it seems is virology.
My question is: Does SARS-Covid 2 pose any health risks to the native bat populations in North and South America? Is there any evidence that humans can spread viruses to bats? Would the native populations have had some exposure to corona viruses already? Would it be like a mild cold for the bats or would it pose a more catastrophic health situation for them?
Many thanks again for giving us all truthful and up to date information and for de-bunking the conspiracy theories. This podcast is a beacon of light in this dark and scary time.
I enjoy the camaraderie and the banter. Please stay safe and please keep on Racon-yelling!
Warm wishes,
Jackie
Dominic writes:
Hey,
Shoot for the moon but 20-30K downloads per episode is amazing for a 1+ hour conversational, educational, non-scripted podcast. You’re doing fantastic!
Just a legislative analyst,
Dominic
Bradley writes:
I enjoy your podcasts but feel you just danced around the problem of the mRNA trial. my concern as an ID physician and recovering vaccinologist is that the immunological mechanisms of protection against COVID are simply not known. The authors are measuring neutralizing antibody which as they point out are correlates of protection. If one would wish to “prove” this (or at least provide more direct evidence) One correct experiment is to take sera from rhesus macaques who have recovered from either COVID challenge or vaccination and inject it into naive macaques and then challenge them with COVID.
I predict based on similar studies being done decades ago on influenza challenge in mice that the lungs would be protected from challenge but not the upper airways (which require mucosal immunity). It was pointed out (I think by Brianne) that mucosal immunity was not measured in the Moderna trial, and I think that’s likely because it is so much easier to measure serum factors. This apparent flaw in their study gains even more importance because it appears that the initial infection with COVID occurs in the nasopharynx via attachment to ACE2 receptors.
What do you think?
Bradley S. Bender, MD
Joerg writes:
Dear TWiVers, no listener question, just a comment on your recent episode:
Thanks so much for debunking (again and unfortunately not for the last time) the hydroxychloroquine BS. Yet again, there was a positive remark: I like the Condit bonmots, I started a collection.
“This is not going away anytime soon. We are still dealing with vitamin C.”
Correct, but vitamin C does not harm as HCQ does. Let the people have their dose of vitamin C, there is plenty of proof of placebo effect. Great if this comes w/o side effects (other than spending a buck or two).
Didn’t want to interrupt your brilliant podcast, so would you please go on
Best wishes,
Joerg
Elise writes:
Dear TWiV,
Thank you so much for my new favorite podcast! I’m a recent listener, and very grateful to have the podcast to turn to as an assurance that I am being told the facts about things that I might misinterpret if I found them elsewhere. Furthermore, as a third year undergraduate biology major with a fascination for microbiology and virology, I love being able to look up to you all as role models.
I am set to move into my on-campus apartment two weeks from today (August 16th) for a mixture of in-person and online classes. Last week I completed the at-home testing kit required for my return. However I think it’s clear that my school–though they are asking us to self-isolate until we arrive–is sweeping under the rug the guarantee that students will be exposed between the time they take the test and step onto campus. As far as I know there are no procedures in place for regular asymptomatic testing upon our return. Knowing how important testing and surveillance is to ensure that we won’t have to pack up and leave as soon as we move in, and also that rapid daily testing tools exist that the school has resources to use, this is frustrating to me. How can I, as a lowly undergrad, communicate the importance of frequent testing to the administration of my school? And is there an avenue by which the school can acquire the rapid daily testing measures despite the fact that they are not yet FDA approved? I feel that without proper testing procedures, the school is taking a risk that is not outweighed by the benefits of being on campus (benefits which will be limited by the fact that many activities will be cancelled). What can I do to show the school that frequent testing is a way towards striking a balance?
Thanks for your advice!
Sincerely,
Elise