
Stephen writes:
Hi Twiv,
TWiV is saving lives! My brother is a virologist who turned me onto this show in early April. I have been listening ever since.
Recently, Over the weekend My wifes aunt went to the hospital with a 105 F fever. She was delirious and had difficulty breathing. She tested negative for covid, but wound up having a substantial amount of antibodies, it appears she is fighting phase 2 covid. She just so happened to be rushed to the same hospital in plainview where Daniel Griffin works.
When it became clear that Aunt anonymous was suffering from phase 2 covid I insisted that my inlaws request Daniel’s care. Hearing his weekly updates made me confident that she would be meeting with the best.
I am happy to share that Daniel did meet with my wifes aunt and now trust that she will be getting the proper care.
Thank you Twiv and thank you Daniel!!
Best,
Stephen
Landi writes:
Hello,
I heard Dr. Griffin make reference to aerosol generation by nebulizers, and I’m aware that the CDC considers it an aerosol generating procedure. The UK National Health Service, however, states that nebulized medication administration is not an aerosolizing procedure because the aerosol generated is not from the patient but from the machine; they don’t provide a reference, though. I’m curious what you think about their argument? Especially as we have more pediatric patients with the disease, it may be hard to get cooperation with an MDI/spacer.
Thank you,
Landi Cranstoun, MD
Sangeeta writes:
Hello there
I’m so glad I discovered TWIV during this journey of self learning and gathering accurate information in this pandemic. I have recommended your podcast to many physicians and medical students. If there is one podcast every scientist and physician should listen to, then it’s TWIV. I’m a pediatrician in private practice in Texas. My favorite episode has been 640- what an eye opening discussion with Dr Mina.
Questions for Dr Griffin:
1. He mentioned that they have started testing for Covid in the patient exam rooms. So far, we have been testing everyone in our parking lot. But as you can expect, parking lot is less than perfect for a clinical exam- pulse oximetry doesn’t work outdoors, neither does the touch less infrared thermometer. If we were to bring these kids to the exam room and do the test wearing PPE, do we need a negative pressure room (we don’t have one)? Would a good HEPA filter help? Or should we just clean the room thoroughly after the patient leaves?
2. Any recommendations on stopping estrogen containing birth control in teens with risk factors for COVID? Estrogen creates a hypercoagulable state but so does pregnancy.
Thank you again. Hope to hear my answers next Sunday
Sangeeta Elhence, MD
Lake Lewisville Pediatrics
Matt writes:
Hi TWIV,
I have loved your zeal for rapid testing since Michael Mina came on (TWIV 640), but a slight clarification on one point. TWIV 647 Rich talked about Abbott ID now and said it uses LAMP. This is incorrect. The isothermal method the ID now uses is called NEAR (Nicking Enzyme Amplification Reaction). As Abbott uses it NEAR uses a pair of primers which introduce a recognition site for a nicking enzyme and their mix has that nicking enzyme in addition to the DNApol, and Reverse Transcriptase for RNA targets like SARS-CoV-2.
LAMP methods currently with an FDA EUA include Sherlock (May6), Color (May18), Seasun (May21), UCSF/Mammoth (July9)
Figure 2 of the paper at the link below has a nice overview of the various isothermal amplification options
https://www.sciencedirect.com/science/article/pii/S0167779911000187?via%3Dihub
—
Matt McFarlane
7 years isothermal amplification and diagnostic
Seweryn writes:
Dear TWIV Collective,
While listening to episode 645, a comment by Brianne and Rich on interpretations of detecting flour and Rich’s DNA triggered a memory, which then also begat a question.
So the memory:
Back in the day when unbiased next-generation sequencing was just taking off, I was working in a 50-year-old research building and decided to have a bash at the technology by sequencing some clinical samples and environmental swabs from around the lab. The data that came back was quite a surprise to me – in among all of the human DNA and other more pedestrian sequences, there were sequence signals for HIV prophage, various caterpillar viruses, and vaccina virus to name a few. When looking more closely at the sequences, it became apparent that they all aligned on top of each other in very defined sections of the virus genomes, suggesting what we had sequenced were either PCR or cloning products, or expression vectors. Now none of the clinical samples were expected to have these viruses, nor did our lab work with such organisms. And this is where working in an old creaky research building comes into play – while our samples should not have contained these viruses, and we did not work with them ourselves, previous tenants of the lab, the other labs on that floor and the one below it had in the past 15 years worked with HIV, lentivirus expression vectors and vaccinia-based vaccine research. So what we had unwittingly sequenced was the work history of the building. The point is this: DNA contamination, especially the amplified fragment kind, is VERY hard to get rid of, and that is why the gold standard for diagnostic PCR workflows involve unidirectional physically isolated workflow areas from clean reagent rooms all the way to “dirty” post-amplification rooms.
Now my question – The presence of RNA in various bodily sites/fluids has been an oft-discussed point of distinction from actual virus on TWIV over the years, only made more prominent by the current SARS-CoV-2 diagnostic dilemmas. But where is this orphan viral RNA coming from? The general dogma of RNA is that it is fragile and easily destroyed, so one could imagine that naked viral RNA in stool/blood/respiratory mucus would get quickly degraded. However this does not appear to be the case. So is there a reservoir of viral persistence that slowly ticks away dribbling out RNA, or is there a more interesting fundamental mechanism at play waiting to be discovered?
Regards from a “wintery” (20C) and so far COVID-19 spared Queensland,
-Seweryn
Seweryn Bialasiewicz, PhD | Senior Research Fellow
Australian Centre for Ecogenomics | The University of Queensland
Kathy writes:
Hello Vincent, Rich, Kathy, Brianne, Dickson, and Alan (I think of you all as the MIghty Twivers 🙂 ) —
Greetings from Seattle where it is currently 18 degrees Celsius at 9 a.m.. We don’t get a long summer here in the Pacific Northwest, but right now it’s beautiful, sunny, and going to be warm, and when summer comes and the rains dry up it reminds all of us why we all live here.
Since Vincent was talking about the TWiV masks and merchandise, I thought I’d send you a silly picture, since I have two sweatshirts, two masks, and a mug (I’m still waiting for that “countering a miasma of anti-think” t-shirt hint hint!). I’m happy to support you guys because I get endless joy, knowledge, and entertainment listening to TWiV (and your other podcasts) almost daily. I myself am a former chemist and retired last year from engineering IT, although I have to admit that I am a frustrated doctor as I love medicine, and am kicking myself for not going to medical school when I had the chance (long story). At any rate, you guys have rekindled my love of science and I’m now reminded of how much I loved microbiology when I was in college. It never occurred to me to enter virology as a field but after taking Vincent’s awesome virology class online, it’s making me want to consider at 61 going to graduate school and becoming unretired lol! I am also nearly blind as a bat from a genetic retinal disorder (sadly, I am not one of those who can do echolocation!), so I doubt that is going to happen, but maybe next life. 🙂 My next door neighbor is a retired infectious disease microbiologist and so we regularly nerd out on all things SARS-CoV-2, Nipah, Dengue, whatever the topic. Life is for learning and thank you all for helping me continue to do that. Thank you also for the laughter and for being a bright light of knowledge in a world where disinformation and anti-think is so prevalent.
Peace and be well —
Kathy
Anonymous writes:
On TWIV 644, you expressed frustration that Pfizer/BioNTech was testing a vaccine candidate that contained only the receptor-binding domain of the SARS-CoV-2 spike protein rather than the entire spike (or other viral proteins). I just wanted to note that Pfizer/BioNTech’s strategy actually involved testing four different RNA-based vaccine candidates – two encoding just the spike RBD and two encoding the full-length spike.
On the show you were talking about preliminary results for BNT162b1, which does encode just the spike RBD, but BNT162b2 is also currently in trials and it encodes the full-length spike protein. The plan seems to be that they will evaluate antibody and T-cell responses in Phase I/II trials and based on those results, one of those two candidates will move forward to a Phase III trial. I’m not sure the status of their other two candidates, but I believe they are also in human trials.
Below are a couple of sites with information on these vaccine candidates along with an excerpt with some of the key details.
BNT162 SARS-CoV-2 Vaccine Program
https://www.precisionvaccinations.com/vaccines/bnt162-sars-cov-2-vaccine
—
BNT162b1 and BNT162b2 are both nucleoside-modified RNAs, formulated in lipid nanoparticles.
BNT162b1 encodes an optimized SARS-CoV-2 receptor-binding domain (RBD) antigen, while BNT162b2 encodes an optimized SARS-CoV-2 full-length spike protein antigen.
In an ongoing Phase 1/2 placebo-controlled, observer-blinded clinical trial, nucleoside-modified messenger RNA vaccine candidate expressing the SARS-CoV-2 receptor-binding domain (RBD) is being evaluated in 45 subjects. This study was last updated on June 29, 2020.
Two of the 4 vaccine candidates include a nucleoside modified mRNA (modRNA), one includes a uridine containing mRNA (uRNA), and the fourth vaccine candidate utilizes self-amplifying mRNA (saRNA). Each mRNA format is combined with a lipid nanoparticle (LNP) formulation.
The larger spike sequence is included in two of the vaccine candidates, and the smaller optimized RBD from the spike protein is included in the other 2 vaccine candidates.
—
Pfizer and BioNTech Granted FDA Fast Track Designation for Two Investigational mRNA-based Vaccine Candidates Against SARS-CoV-2
https://apnews.com/c7c691db3ea74a20bd00f908246f37fa
Just a quick follow-up to this to mention that Pfizer/BioNTech has selected BNT162b2, which encodes the full-length spike protein, to move forward into a Phase II/III trial. BNT162b1, which encodes just the RBD of the spike protein, does not appear likely to be tested in a Phase II/III trial, although they will continue to collect data from the Phase I/II trials of all four of their vaccine candidates. Here’s a link to the press release with more details on the rationale for choosing BNT162b2:
Thanks for all your work on the show!
Best wishes,
Anonymous
Jess writes:
Hi TWiV Team!
Per the most recent episode about science writers and journal pre-prints I’m curious about the route one follows to become a science writer. That’s been one of my favorite parts of my career in science is how to re-package science for general consumption but I don’t know how to end up in a career doing that. Any ideas? Alan?
Thanks as always for your podcast for disseminating scientific information in an equally-effective medium!
Take Care,
Jess
Wayne writes:
Hi Twivers of Truth,
36C here raining and mosquitos galore.
Another email from Japan…sorry for so many but TWiV is a life savor for me…the amount of bogus information out there on COVID is off the charts.
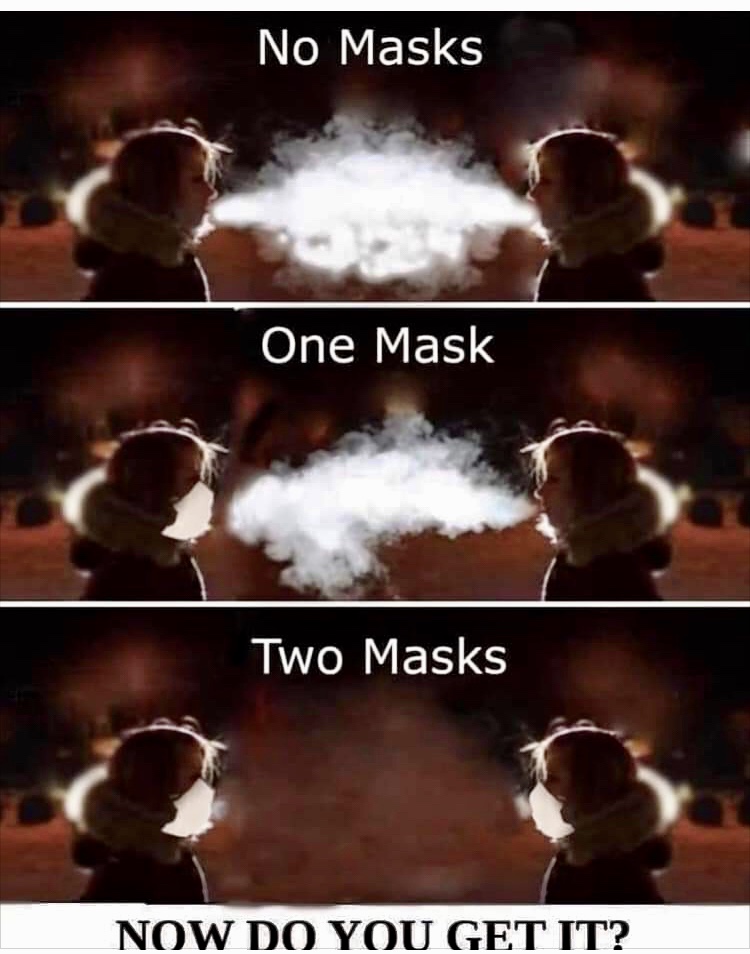
Back episodes ago Dr. Condit commented on how exhaled breath can be seen in Winter…some thing I teach my English students here in Japan on the importance of wearing a mask.
I found this photo that illustrates the exhaled air and the importance of wearing a mask
using cold air to show the importance of masks.
Haiku…
The rain of truth,
leaves now shimmering…
Washed clean!
Best to all,
Wayne
Wakayama JP
Igor writes:
Dear TWiVers,
Thank you for your work. I’m a physicist at UC Davis and I have been following TWiV since episode 601 with Christian Drosten. I moved to California from Germany last year and have been listening to each episode of Drosten’s “Das Coronavirus Update” which is extremely informative but less fun than TWiV. Since “Das Coronavirus Update” is currently on vacation, you have become my primary source of reliable information.
Now coming to stool, which was discussed in TWiV 645, again. According to this nature paper co-authored by Drosten https://www.nature.com/articles/s41586-020-2196-x (Fig. 1), viral RNA is present in high concentrations in stool over three weeks after infection, but it is negative in culture, so stool is fortunately not infectious! I think this is important information for cleaning personnel.
I was very excited by TWiV 640 with Michael Mina. I hope the UC system will start working hard in this direction to implement widespread and frequent antigen testing. Cases are increasing. We need it.
Great thanks to you, Drosten and the other great virologists that enlighten the darkness.
Best,
Igor
Tony writes:
i like the q&a portion of TWiV.
i have a question i’ve not seen addressed elsewhere:
1) what do you, as experts, think of the possibility of mass immunization via “semi-controlled exposures” (eg Pox Parties) for the Coronavirus given that the level of exposure seems to dictate severity of later infection?
I have my suspicion that once the public has a better understanding of the epidemiological facts of the virus and increased lock-down fatigue it will become fashionable to become infected to get back to work (and play) and to protect one’s children.
Thanks.
Rodrigo writes:
Dear Vincent and Crew!
Thank you again for all you do!
On the subject of Mina etal’s testing idea, may I suggest that the way forward here is actually 4 well placed phone calls in sequence (and not necessarily a writing campaign)?
With summary video on hand (e.g., MedCram’s), you guys call Fauci (probably a very brief call) or someone that can call him, Fauci calls and explains it to Pence, Pence TELLS Admiral Giroir (the guy in Charge of Testing) to GET IT DONE, and it gets DONE. Considering the staggering clarity of the argument, the simplicity of the test, the side benefits of school openings, saved economy, etc. this would be a no-brainer to everyone and all involved on the call chain.
While many causes greatly benefit from active public support, letters to Congress, etc., this seems to me is an obvious solution (in retrospect) to avoid a Meteorite that is just about to hit Earth. There is no need to rally popular support on a newly discovered obvious solution to a monumental threat. With your wherewithal, please find the 4 degrees of separation to the authority in charge, and just get it done.
With deepest thanks,
Rodrigo
Kevin writes:
The TWiV crew
Greetings:
May I suggest that the letters not be restricted to just political leaders. Consider your local news outlets: TV, newspapers, and radio. Research the reporters filing the most SARS-CoV2 stories and communicate directly with them. Wouldn’t it be great if questions about cheap, rapid testing started to be asked at every news conference?
Love your podcast, keep going, please
Anon writes:
Hi all,
I was hoping you would comment in your podcast about this article that just came across my twitter feed, about a DIY vaccine that was developed by Preston Estep, and taken by at least 20 volunteers, including George Church (he of mammoth cloning fame).
https://www.technologyreview.com/2020/07/29/1005720/george-church-diy-coronavirus-vaccine/
I am not a virologist, immunologist, or someone who studies human disease, but as a scientist (I study permafrost and Arctic ecosystems), this strikes me as reckless, dangerous, and counter-productive. It sounds like there are problems with the basic science of it, that I only have a limited understanding of, but even without that some basic questions come to mind: How will they know the effectiveness of this vaccine? Its safety? How could it possibly be scaled up to produce hundreds of millions of doses? Have these people ever taken an ethics course or learned anything about experimental design???
Would love to hear your thoughts in more detail.
Thanks!
(I’d prefer to stay anonymous)
Ginny writes:
I love TWiV and recommend it to everyone. I contacted my electeds about the 10-minute test. Sen. Schumer’s office sent me back a form letter about what he’s doing about COVID, so I’m not sure they understood. I’ll have to try again.
You were talking in #647 about COVID transmission from children. I had seen something on this earlier from the University of Vermont. The sample is very small, but it also references work from other countries.
Even if children didn’t often transmit SARS-CoV2, since there are many adults in schools, in my opinion it’s still risky to open schools without the consistent, universal testing that Dr. Mina described.
Thanks for all you do.
Stay safe-
Ginny
Rocheter, NY
Amanda writes:
Hi TWIV team,
I’m writing to you from Santa Fe, NM (from whence last week’s Opera letter writers also came – who knew that a tiny town renowned for its art would have such secret virology enthusiasts!)
I am only a training director for the national weatherization program, located here in Santa Fe. After several months of listening to TWIV I realize how little I know about viruses, but also how much more I do know now compared to my non TWIV-listening friends. Thank you for this wonderful gem of a podcast.
My question is about the news yesterday that Dr. Fauci mentioned wearing goggles for added protection against the SARS CoV-2 virus. The program I train for sends workers into homes to help with energy efficiency measures. There is now very detailed safety guidance for these workers, but one thing that has not been stressed is the wearing of safety goggles. Of course, most of the people doing this work already have safety goggles they may wear to protect themselves from dust etc. where necessary. Do you think it would be good advice to just have them wear the safety goggles all the time when they are in other people’s homes?
Thanks again for all your time and expertise which so many of us are benefitting from immensely.
Amanda
Mark writes:
Hello TWiV team,
Mark, here. The electrician from episode 629, I’m sending in a copy of the letter I shared to my county and state officials to you all. I actually got a response!! And not a copy paste version, a real email from an actual person who took the time to read what i wrote and looked into the study from Michael Mina! I was blown away and ecstatic to get a response, it gives me hope that there is a small chance something can change, maybe. Here in Maryland we seem to have a pretty level headed governor (Hogan) and open to new ideas to get things moving again. I’m hoping that the study from Michael will be able to reach him and our public health officials. Fingers crossed.
Thank you, for creating such a fantastic podcast that allowed me to be just knowledgeable enough to be heard, with a glimmer of hope, to change the way things are working out during the pandemic. I’m pasting the letter I wrote below, to actual scientists and Drs., my email is most likely a disaster, so if you read it….be gentle! haha But it got the message across and that’s what we need.
Side Note: In TWiV #629, Alan, Vincent and Dixon read my letter and told me to keep spreading the information I have to my fellow layman construction workers and veterans. Since i’m not in “The Ivory Tower” and may have a platform of sorts, given that my wife is an immunologist and helps me translate/understand….OMG was this wrong! LOL. It’s amazing, some of these people are so far gone! I’ve been able to get through to a few of them (Which is good) but the majority say that i’m just part of the “Narrative” and “Agenda”, creating more brainwashed “sheep” in America Hopefully it at least gets them to think a little, or start to doubt what they think they know.
Anyway, here’s the letter to my officials. Again, be gentle .
“Governor Hogan,
I am writing to you in regard to current coronavirus testing and capabilities. I know the majority of your job is comprised of people coming to you with problems and zero suggestions and/or solutions. I have attached what I think is a potential solution. A recent study/preprint that has been released from the Harvard School of Public Health for peer review along with a podcast about viruses—the podcast is hosted by a PhD virology professor (Vincent Racaniello) from Columbia University and other researchers and professors.
Just last week their guest was a man named Michael Mina from the Harvard School of Public Health. Michael and his colleagues have come up with a pretty ingenious plan to combat SARS-2 testing quickly, efficiently, and financially viable. Currently, the testing around the United States has been —for lack of a better word—terrible. The need for specialty equipment and BSL-3 labs to conduct the testing has caused results to take too long to put a dent even remotely in trying to control the spread of infections in addition to being expensive. Thankfully, Maryland seems to be doing a bit better than a large chunk of the country, but we can do better, and obviously the country can as well—especially given the lack of interest and leadership coming from the top.
The model of the attached testing plan is to have cheap, easily, and quickly made tests that could potentially be around $1 per test; they accomplished this by creating a test that has a lower sensitivity than what has currently been the main focus of the FDA, but also being able to test more frequently. Employers, schools, restaurants, manufacturing plants, and even individual households would be able to conduct these tests to catch infections of SARS-2 every day at or before their highest viral shedding stages of infection. It is true that the chances of a false negative test are greater with this model; however, by being able to test every single day or even every two days, the chances of having two false negatives is drastically reduced. The lower sensitivity of this model is mainly observed at very low viral loads of infected individuals but equally as sensitive as the current tests available during the height of infection and shedding. Even if the small chance of having 3 consecutive tests were to happen, that is still only 3 days of an infected person shedding a virus compared to the current 8 days that it is taking to get PCR test results due to backlog. PCR testing also has its own downfall in the fact that they are looking for RNA—not necessarily viral RNA. Conducting PCR tests is also not overly efficient at deciphering infectious RNA from inactive RNA bits and pieces—which is also holding admitted patients in hospitals that could potentially be ready to be discharged but cannot get a negative PCR test.
Naturally, logistics must be sorted out to begin producing this test; I do not have the answers or connections to be able to assist with this portion; however, given that the test could be as simple as a strip of paper with antigen, it could essentially be easily made by local paper manufacturers with the help of the state governments to modify their existing equipment to add this antigen to the paper that they would already be processing. I think that the proof is out there that people and businesses are willing to assist with the pandemic in their own way just by seeing examples such as breweries and distilleries diving in headfirst to produce sanitizers. I have no doubt that there are more people out there ready and willing to do the same.
The main problem that the preprint is having currently is getting it noticed by the FDA for testing and approval. The FDA is determined to not see beyond the currently funded tests—which have shown to be cumbersome, slow to produce, and slow to analyze. I personally think that by even abandoning the money that has been spent on the current tests at the FDA, this new test could be picked up, approved, produced, and circulated cheaper than what has already been spent on the current tests.
Thank you for your time and consideration. I hope you are also able to find the time to listen to the first 30 minutes of the attached podcast, where Michael Mina explains everything that I just wrote—but better.
I am writing this to you with no political agenda—just as a concerned citizen trying to keep up with the science. “
James writes:
Hello TWIV,
Really love the show. I’m wondering if you can talk about how the phase 3 vaccine trials, pfizer/moderna etc, are designed? Specifically how do they control for the random exposures out in the world between the 2 treatment groups? I’m guessing that the large number of subjects, 30,000, provides enough power to overcome this?
Thank you
Christian writes:
Dear TWIVonians,
I have been an avid TWIV listener since the large Ebola outbreak starting in 2014. Let me briefly mention that I greatly enjoy the weather reports and especially the banter during the show. Obviously, in the current pandemic I have mostly kept my TWIV listening habits and consumed the excellent info conveyed so clearly (including the recently aired interview with Eugene Koonin, although I am only a 3rd or so through. As a fellow scientist I am really impressed how thoughtful he is and also by the precision of his diction.)
What I really wanted to ask about is the ‘new testing paradigm’. As Vincent calls it “I have drunk the Michael Mina Kool-Aid”* and am fully onboard with the arguments. However, my experimental scientist experience suggests that although the principle seems completely sound there could be little devils in the implementation details.
Please do not misunderstand this as a criticism of the approach, rather I was wondering if somebody is looking at running what I may call, as a non-expert in the area, a large scale trial of the concept, e.g. using a rapid test everyday on everybody in a certain community that signs up for it. This would help uncover implementation issues and, I am almost certain, prove to the doubters that this can be made to work and work well. I am not sure what the ‘control’ would be or how the ‘trial’ would be evaluated, so these would be interesting points of practice. A trial would also hopefully dispel a possible argument that Mina et al’s work is “only” a simulation study, since some people like to discredit anything that is not actual data based (even though the simulation IMHO is very sound and straightforward plus based on solid assumptions that are themselves based on data).
Would be great if you could discuss this and perhaps there are already efforts under way that you are aware of?
Keep up the excellent work,
Christian
* when I looked up “drinking the Kool-Aid” on Wikipedia I saw that “the phrase often carries a negative connotation”…
—
Prof Christian Soeller – Prof of Physical Cell Biology – Living Systems Institute & Biomedical Physics – Univ. of Exeter
Shree writes:
Hello TWIV!
I have been hearing about all the new sars-cov-2 vaccine candidates being developed at “warp speed.” What does warp speed actually mean? The NIH website says “Protocols for the demonstration of safety and efficacy are being aligned, which will allow the trials to proceed more quickly” – but aligned is a very broad and non-descriptive term. I’m curious to hear your discussion on the safety/efficacy feature of warp speed.
Thanks! And thank you in general for this spectacular podcast (I’ve been listening since I started grad school 6 years ago, and bug all my friends to listen to it too).
Shree
Too bad Spock is no longer with us! He would have given a good summary of the WARP concept- ddd
Wendy writes:
Resending both so I don’t get Raconielled-at for mailing to his personal box, and, because I want to make sure the entire team gets my thanks and request/recommendation re:TWiV-branded chairs!
Also, omitted my weather update – outside Denver, CO where it’s an actually tolerable 93 F, brown-grassed, dry heat Colorado day with a chance of our politically unusual and frustrating ”Democratic-Libertarian” Governor possibly (but not likely yet) making a needed move toward curbing our rapidly trending numbers and a loud-as-thunder, recentLy mandated outdoor masking in my county. Yippee! I’ve concluded that Libertarian Leadership is an oxymoron. It’s all too much, “have your cake and eat it too,” no-decision, decision- making. CO has a great economy, it’s important and it would be wonderful to maintain that – but I don’t know how he thought he’d do so given predictable in such a counter-cultural, “freedom”-driven state without making some clear and politically/economically painful decisions upon reopening. So now…we continue to climb. Not terribly, but not as well as we could be doing. We consistently have visitors from CA and TX because all of our parks and mountain towns are open for business. I’ve seen the plates myself. So many in fact that when my husband lost his road-ID bracelet on a mountaintop recently, it was recovered by someone from out of state. They apologized sheepishly about just needing to get away… So disappointing. Anyway, unnecessary and off-topic tangent! Grrr!!
Re: end of ep 642 (love this episode name)
A. Thanks for bringing Racanyelling to the world, and to all of you, for my “moment of zen” – well, my long moments. My husband said he didn’t know how I could listen or watch repeatedly to two hours at a time of variations on the same arcane subject … to which I replied, “Yeah, it’s not like listening to (Grateful) Dead show or anything – variations on the same song, over and over again, accompanied by intense fandom, and memorizing arcane data” boom. So, thanks for that opportunity.
And – B – my main reason for writing – have you thought about a line of TWiV chairs, I wonder… as I outfit my daughter’s remote schooling set-up and actually realized I‘ve been debating between a gaming chair and one that looks like yours and Dickson DesPommier’s (sp?)…. I would buy those. And they’d get used both for great back support while watching y’all or the Dead on YouTube.
Thanks much, for all you’re doing.
PS – my daughter and I’ve already had CoVid – my husband no symptoms, my daughter (12) “CoVid toe,” lightheadedness, vasculitis and lack of circulation to one foot – looked similar to Raynaud’s – some neuropsychiatric symptoms that had to be treated for a few days – (a hypomania/anxiety) and fatigue. Major symptoms lasted for her 5 weeks. I had close to 90 days total, the worst only about 2-3 weeks of chest/lung pain, SOB, hypoxia…all treated at home because this was early enough that our symptoms were “atypical” and even I had a hard time believing the diagnosis, despite understanding much of the sequellae and testing issues. Plus, that was the recommendation at the time. Due to supply issues, I didn’t get a pulse-ox until the end of the 3rd week – as respiratory symptoms were improving. It was alarming to see I was consistently getting O2 readings between 88-92, with a heart rate as high as 170 just standing up. I ignored these because I was *improving* and my physician didn’t notice “blue lips” via telehealth, so, everything must be fine….. We made it. All is good. It could have gone differently for both of us and I’m glad and impressed at the speed of information gathering and reaction worldwide. Really a heroic effort, in just horrifying anti-science, anti-information/intellectual climate. Thank you, for being a life raft – all of you.
PPS – like that great hair stylist who wrote you, by virtue of demographics I’m surrounded by conspiracy theorists, amateur astrologists, and anti-vaxxers/maskers. CoVid partiers.
Again, horrifying – but also, sociologically fascinating. Medical Anthropologists/Sociologists will be dining out on this for a long time. I need my TWiV gaming chair so I can sit back and watch – from a distance!
Thanks again,
Wendy