
Thomas writes:
I am an adult cardiologist in the Philadelphia area with a four-year-old son. In early February this year, my four-year-old tested positive for influenza A and three days later, after persistent fevers, was started on a cephalosporin for bilateral otitis media. He completed a 10 day course of the antibiotic without incident. Then, about four days later, around the last week of February, he developed a terrifying constellation of symptoms that I had never seen in him before, not being a pediatrician. His hands, feet, knees, wrists, elbows became swollen, red and very painful to the point where he could not walk or even fit into his shoes anymore. He complained of a headache and a stomach ache. He broke out in a rash all over his body that did not quite look like hives. He spiked a fever. The symptoms persisted for about a week. Covid was supposedly not yet in Pennsylvania, and the pediatric emergency doctor diagnosed him with serum sickness from the cephalosporin at that point. But I wonder if it is possible that he actually had Covid and then multi system inflammatory syndrome?
Now that we know that this coronavirus was present in the population much earlier than previously thought, what is the likelihood that it was present in Pennsylvania in early February? Is there a way to determine whether strange cases like this actually represented MIS-C? (is the antibody test of any use at all at this point? ) And what are the recommendations for following children who may have had MIS-C? Do they need to see a pediatric cardiologist? Pulmonologist? Rheumatologist?
Kids survive, but for some of them this is just the beginning… Thank you for sharing your knowledge and brilliance with the world. We need so much more of it!
– Thomas
Ewa writes:
Dear TWiV,
I am a pharmacist and medical journalist from Sweden, and I currently work to write texts about covid-19 for a digital care giver, including texts about interpretations of serology results.
I regularly listen to your pod and usually write a summary of Daniel Griffins part for the physicians that are too busy to listen for themselves. I was a bit intrigued by some data from yesterday. If I heard/understood correctly, Daniel Griffin said that serology starts trending down, and (at about 6 minutes in) “If you look at people two months out, everybodies antibody levels are trending downward, and if you look at people with more milder disease, maybe 40 percent are now serology positive, people who were sick enough to have high antibody titers, you start to see them turn serology negative.”
https://www.nature.com/articles/s41591-020-0965-6
According to this source: Forty percent of asymptomatic individuals became seronegative and 12.9% of the symptomatic group became negative for IgG in the early convalescent phase.
I just want to make sure that I understood and pass it on correctly, could you help me find out if Daniel Griffin has another source or if he meant to say serology negative?
I also want to send my warmest thanks for a great pod, and that we really appreciate Daniels updates, you are all great.
Best wishes,
Ewa
Richard writes:
Dear Twivers, Ivermectin was addressed in an earlier TWiV episode. It is apparently being used extensively in South America and Asia. Please comment and ask Dr Griffin if he has any take on use of this medicine for C19.
Thank you,
Richard
An Upset Chinese Listener writes:
Dear TWiV team,
I was looking for how American virology scholars were dealing with this pandemic, and the TWiV special with Ian Lipkin brought me here.
I was listening to TWiV 637 and at the very beginning you were talking about how China approves Ad5 vectored SARS-CoV-2 vaccine to only the military, and some of your comments really infuriate me.
You said that this is Phase 3 test, which I agree, but then you folks went on to say how it’s like treating the soldiers as some kind of test subjects, bringing up how the US military would follow CDC guidelines.
I’m sorry, but this is just bigotry.
Have you ever considered the possibility that:
1. We already have this thing under control domestically, so we don’t have a population to test the vaccine.
2. Global travel is rare, and fully quarantined.
3. The military are basically the only people who have to make contact with foreign individuals in uncontrollable environments.
I also follow opinions on our social network. Virology related students and professionals. Most of them have another angle on this subject:
That the Phase 2 probably proved this thing’s quite safe. And since we have Indians attacking us for nationalist reasons, and we have some military overseas, them taking this virus is likely to be better than nothing, while fulfilling some Phase 3 testing purpose also.
According to some people, we are doing tests with countries like Brazil, etc. where the virus is still running rampant.
The fact that you didn’t even think about other possibilities and goes directly to “Chinese people have no human rights” default rhetoric is just bad quality for a scholar.
“One Child Policy” remember? Even if you don’t think we have human rights, you think the soldiers’ parents would just let their only child be lab rats?
The fact that we shutdown our economy when we had only thousands of cases should be the proof of how much we care about human lives.
Hope we can have an exchange on this topic.
Thomas.
P.S. Since I’m already here, why not add in a bit of a rant?
IMO, failure in handling the coronavirus in the US is a systematic failure. No one is really innocent.
I watched in shock as Fox News brought in a “doctor” telling people masks were not important.
CNBC used to follow every Chinese Covid news with “if you believe their data”.
Even you guys, back in TWiEVO 52, were acting like this is no big deal, and that was freaking February 26th!
How could the scholars only blame Trump when the entire society had been receiving false information?
And how are you suppose to train America’s future generation of virologists when you are still bigoted even after you were part of the problem?
Corvin writes:
Hi Twiv team,
I wonder if you’ve seen Yale’s reopening plan? It seems pretty good:
https://covid19.yale.edu/health-safety-guidelines
Thanks
Corvin
Peter writes:
Butterfly alights
TWIVian wings’ gentle dance
heals virus worn Earth
you guys keep me sane. God Bless!
Peter from Miami
Nicholas writes:
The people who like the finer division of Fahrenheit have a point. So my proposal is this:
Just multiply Celsius by 2.
Mary writes:
Dear TWIV-ers,
I write to you from the Detroit suburbs, where the effects of climate change are apparent as it is 92 F at 2 pm today and we’re having a week of nearly record high temps in the mid-90’s. This is about 10 degrees above average.
In response to Anonymous’s letter in Ep. 629 re: what explains the outbreak in hot and dry Arizona, you failed to consider one option: Perhaps it is the case that we humans are protecting the virus from the hot and dry weather. When the virus is inside a human (perhaps someone who brought it to AZ from another, cooler state), it only needs to endure approximately 98.6 F while that human is asymptomatic. When that human is outside, the virus stays comfy in its 98.6 F home (though any virus expelled through breathing, etc., might die in the heat and dryness). However, when that human is indoors, the temperature is likely much cooler and any virus escaping will do just fine, especially if it is lucky enough to find its way into another human. And so it goes.
This puts me in mind of another letter you recently read inquiring whether air conditioning might increase transmission somehow. It might be the case that what causes humans to use air conditioning (hot weather) also causes them to spend more time indoors and it is that increased time indoors that results in more cases.
Love your show, especially the banter. It is the banter of creative, nerdy types. I was turned on to your show by another creative nerd — Mike Pesca (of The Gist podcast fame). Long Live TWIV!
Cheers,
Mary
Jim writes:
Hello TWiVniks!
A loverly 92F/33C/552R/306K here in St. Louis, former home of the bowling hall of fame. This paper on medrxiv caught my eye, and I immediately thought “I wonder how Brianne’s campus might institute this?” just as a thought experiment. I went to a small Midwestern school (go Illinois Wesleyan Titans!) of about 1900 students, and think it would be possible, but challenging to implement there. UW-Madison? Forget it.
Thanks for all you do! Really enjoyed TWiV #636 — lots to learn there. My wife (wrestling with teaching Philosophy in the fall) asked me the other night night if I was going to “twivit”.
“Twivit?” I asked.
“Yes, isn’t that what you do when you go out on the deck with your headphones in the evening? Listen to twivit?”
“The podcast is called ‘TWiV’, This Week in Virology, and yes, that’s what I’m doing.”
“Oh,” she said. “What’s a twivit, then?”
I don’t know, but I think it’s something Elmer Fudd places hot casserole dishes on so he doesn’t scorch his countertops.
Vewey funny! ddd
Barbara writes:
Dear Vincent and TWIV Team,
I thought you might like to meet Kid Covid: http://kidcovid.ca/
‘Kid COVID Fights Back!’ is written and illustrated by Guelph, Ontario, Canada artist, Barbara Salsberg Mathews. It is a wonderful, free resource for kids and parents to better understand and protect themselves from SARS-CoV-2. It has been distributed around the world and added to the New York City Department of Education’s on-line library of free COVID-19 resources for children. For a quick video overview of the book: https://www.instagram.com/p/B_0vnJKAo6Q/
It may be of interest to you and/or your listeners.
My best,
Barbara
River Road Creative
Edward writes:
Hi TWiVers,
Given all the bad decisions made by sports organizations that have (justifiably) brought out Vincent’s inner grump, I thought I’d share a nice ray of sanity from the roller derby community:
https://static.wftda.com/files/covid-19/WFTDA-COVID-Return-To-Play-Plan-v1.pdf
The Women’s Flat Track Derby Association released it’s Return To Play Guidelines a little over a month ago, which features a seven-tier ladder which includes guidelines for not only when to advance, but when to back off based on clear health metrics. We even got a nice little write-up in WIRED:
https://www.wired.com/story/womens-roller-derby-has-a-plan-for-covid-and-it-kicks-ass/
I’ve been enjoying TWiV (and the occasional TWiP) since April, and found the Singapore discussion on Dengue to be particularly fascinating.
Thanks for all you do,
-Edward “Bit Shift” Adams
(Just a roller derby referee)
Andres writes:
Dear Twiv team,
I have been listening to your podcast since before it went mainstream, it was first introduced to me in my virology class by Dr Moriah Szpara and Dr Craig E. Cameron. Currently, I am just a PhD student in Cancer Biology, but we used viruses as another tool in our research. You guys have inspired me to do my own science podcast, keep the good work.
I have two questions
1-Vincent your lectures have been excellent, they have served as a great review and I am learning a lot of new things. Would you consider releasing your exams eventually? for those loyal listeners of your lectures that will like to test what they have learned.
2- It seems to be a relationship between the insufficiency of Vitamin D and severity of COVID-19 or other viral associated lung diseases (1) (2), while this is not a one variable effect, causation has not been proved and other factors remain important, some studies point in the direction of being another important co-factor in the severity of the disease(3). Vitamin D is an important hormone involved in many biochemical processes, that decreases with age, diabetes, obesity and is produced in fewer amounts in people with more pigmentation (4)) ( another variable of why certain races are affected disproportionally not only in the US but in other countries in northern latitudes (5) (6) where medical access is not an issue like UK or Sweden).
In many countries including those a bit warmer, people are vitamin D deficient because of modern lifestyle or excessive use of sunblock (7). In the winter months, this is worst, and it affects in greater amount those of African descendance living in northern latitudes countries (for example Somalis in Scandinavia (8)(9)(10)). Vitamin D is cheap, safe, and easy to take but it seems many people do not take it. What is your general opinion about this, and should authorities put a bit more emphasis on supplementation as a preventive of severe outcomes?
Best Regards,
Andres
1-Grant, W. B., Lahore, H., McDonnell, S. L., Baggerly, C. A., French, C. B., Aliano, J. L., & Bhattoa, H. P. (2020). Evidence that vitamin D supplementation could reduce risk of influenza and COVID-19 infections and deaths. Nutrients, 12(4), 988.
2-Bajwa, E. K., Bhan, I., Quraishi, S., Matthay, M., & Thompson, B. T. (2016). Low Vitamin D Status Occurs In 90% Of Patients With ARDS And Is Associated With Longer Duration Of Mechanical Ventilation. In A53. RESPIRATORY FAILURE: RISK FACTORS AND OUTCOMES IN ARDS (pp. A1846-A1846). American Thoracic Society.
3- Zittermann, A., Iodice, S., Pilz, S., Grant, W. B., Bagnardi, V., & Gandini, S. (2012). Vitamin D deficiency and mortality risk in the general population: a meta-analysis of prospective cohort studies. The American journal of clinical nutrition, 95(1), 91-100.
4- Clemens, T. L., Henderson, S. L., Adams, J. S., & Holick, M. F. (1982). Increased skin pigment reduces the capacity of skin to synthesise vitamin D3. The Lancet, 319(8263), 74-76.
5- Klingberg, E., Oleröd, G., Konar, J., Petzold, M., & Hammarsten, O. (2015). Seasonal variations in serum 25-hydroxy vitamin D levels in a Swedish cohort. Endocrine, 49(3), 800-808.
6- Panarese, A., & Shahini, E. (2020). Covid‐19, and vitamin D. Alimentary Pharmacology & Therapeutics.
7- Hashemipour, S., Larijani, B., Adibi, H., Javadi, E., Sedaghat, M., Pajouhi, M., … & Hossein-Nezhad, A. (2004). Vitamin D deficiency and causative factors in the population of Tehran. BMC Public health, 4(1), 38.
8- https://www.reuters.com/article/us-health-coronavirus-norway-immigrants/covid-19-takes-unequal-toll-on-immigrants-in-nordic-region-idUSKCN2260XW
9- Godlee F. The burning building. Editor’s choice. BMJ 2020;368:m110110.1136. doi: 10.1136/bmj.m1101
10- https://www.bmj.com/content/368/bmj.m1101/rr-10
Trudy writes:
Dear TWiVers,
In follow-up to your discussion regarding the Spanish study that led journalists to conclude that herd immunity is “unachievable”, I have the following comments:
First of all, the authors admit that “cellular immunity, which was not evaluated here, might also play a role in protecting against SARS-CoV-2 infection.” There are numerous publications and there have been numerous discussions on TWiV about the fact that T cells may be just as important, if not more important than antibodies in protecting against a second infection with this virus. These papers lead to the conclusion that epidemiological data relying only on antibodies may lead to substantial underestimation of prior exposure (or immunity) to the virus.
I would also like to add that although the pandemic was bad in Spain, the mandate for quarantine was put in place in early March and remained as such for quite a while, thus preventing further spread of the virus. So, like Rich, I would not be surprised if the overall seroprevalence in Spain is lower than in other places.
There are also a couple of studies done in Italy that show that up to 74% of infected people can be asymptomatic (with about 45% of those being truly asymptomatic – not just pre-symptomatic). There are many data indicating that people with asymptomatic infection produce low levels or no antibodies at all – but they could still produce T cells. This has also been discussed on TWiV.
Based on everything we know about coronaviruses, there is no reason for us to believe that a first infection with SARS-CoV-2 won’t confer at least some level of immunity against a second infection, and that a second infection will be much milder, if it should occur.
I personally think that the fears about a second infection being more severe than the first are unsubstantiated at this point – there is no evidence for that. While this phenomenon is known for Dengue virus infections, to my knowledge there is no evidence that this phenomenon exists with coronaviruses – in particular with a second infection with the same serotype, but we have plenty of evidence that a first infection confers at least some level of immunity.
On that topic, there are at least a couple of studies that show that rhesus macaques that were infected with SARS-CoV-2 were fully protected from a second infection with the same virus and that this protection was mediated by both antibodies AND T cells. This has also been discussed on TWiV. Admittedly, monkeys are not people, but these results align with what we generally know and understand about immunology and viral infection.
Thank you for ramping up TWiV recordings, I don’t think I have ever learned so much about one virus in such a short time.
Best Regards,
Trudy.
Victoria writes:
Hi there! I’m a student in Caltech’s Bi115 class, where we discuss viruses and their applications to biological systems. I was recommended to check out your podcast (which I do not regret!) and I have a question for you.
In 614 you mentioned that the Kawasaki-like disease that has been popping up might be driven by coronaviruses in general, and not just SARS-CoV-2. I came across this paper from 15 years ago suggesting that “New Haven coronavirus” was associated with Kawasaki disease [https://academic.oup.com/jid/article/191/4/499/937208], and it seems very possible to me that there is something about coronaviruses that leads to Kawasaki-like disease. I know that Kawasaki is a pretty new presentation, but I would be very interested in hearing any thoughts or theories that you might have regarding why there might be an association between coronaviruses and Kawasaki-like disease.
Thanks!
Victoria
Julia writes:
Dear TWIVers,
66F (18C) here in beautiful Southern California, where the setting sun is just lighting the sky on fire.
A silver lining of this pandemic is that it brought me to you! Thank you so much for all the truly excellent content. As a clinician (I am “just” a hospital-based oncology nurse), Daniel Griffin’s updates have given crucial insight into the New York outbreak and our developing understanding of the covid-19 disease process. I also especially appreciate the remarkable guests Vincent has shared with us: Susan Weiss, Jeff Shaman, Kostya Chumakov, Stanley Perlman, Christian Drosten, Doris Cully, Jon Yewdell, Ian Lipkin, Mark Denison, Ralph Baric… Wow, my mouth dropped open writing out the list. What a privilege it has been to hear from these thoughtful experts. I am now a Patreon contributor, and everyone should be. Your content is worth gold in this time of misinformation and mistrust of science. (https://www.newyorker.com/news/news-desk/the-mistrust-of-science)
On to the reason for my email: elaborating on David’s letter from episode 613 about the predictive value of tests. This is a critical consideration for serology assays in light of the “immunity passport” discussion (clearly everyone’s favorite topic, particularly Alan’s, hah). When disease prevalence is low, even tests that look really good on paper have a remarkably poor positive predictive value. In other words, a positive test isn’t very reliable, and in the case of serology, the positive test is the result we’re interested in: who has antibodies?
Why is the positive predictive value low? The only way I could get it through my head was just to do out the math. A few times. Here is an example.
If you have a serology test that’s 100% sensitive, it will correctly identify all people who DO HAVE antibodies and not miss a single one (no false negatives). If that same test is 98% specific, it will correctly identify people who DO NOT HAVE antibodies 98% of the time. Only 2% of the time will the result tell a person who DOESN’T have antibodies that they DO (or a false positive). This sounds pretty good, all in all, right?
Here’s where the disease prevalence throws the wrench in. Say you test a population of 1,000 people, but only 2% of them have actually been sick. The test will correctly identify all the true positives: 20 people out of 1,000. It will also correctly identify 98% of the true negatives, 960 people. But, it will give 20 people a false positive result.
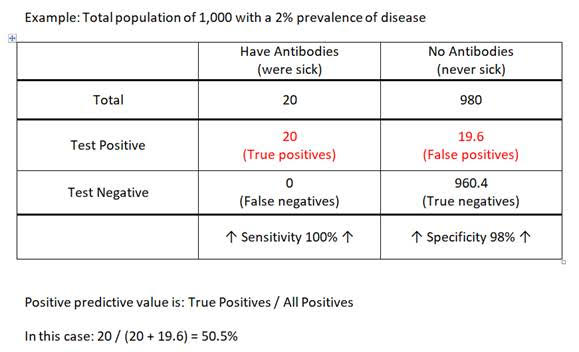
Isolating just the people who got a positive result reveals the problem. We have 20 people who got a positive result and were truly positive, and 20 people who got a positive result but were actually negative. Who is who? The positive predictive value is True Positives divided by All Positives. 50%. A test that’s right only 50% of the time is basically useless on an individual level.
Now, you might point out that the positive predictive value for a test that’s 98% specific increases rapidly as disease prevalence increases. For the example above, at 10% prevalence the PPV is almost 85%. Much better! However, most of us (outside of maybe New York City and a few other places) are probably in a pretty low prevalence area. Spain, one of the hardest hit countries in Europe, just conducted the first phase of a major serology study involving 60,000 randomly selected persons. The average prevalence was 5% (95% CI 4.7% – 5.4%).
And all this leaves aside the discussions of rates of seroconversion, whether antibodies are actually neutralizing, whether they confer immunity, whether that immunity is sterilizing… On and on. The upshot for me? We have a long way to go before any of these results mean anything about who can consider themselves safe from future infection or from being a vector of transmission.
Keep up the great work, please!
Julia
PS – I’m so glad Ori has recovered. I saw on Twitter that he donated convalescent plasma. Will he be back on the show? He was a good addition to the team, I thought. It would also be great to hear from Valeria Cagno again, if she’s willing. I would love an Italian/European update. I tried to listen to her podcast, Scientificast, but my Italian is not quite up to par.
Eric writes:
Dear TwiV team:
I watched all the 2020 lectures from Vincent’s virology course. It was fascinating. Here’s what I learned:
1. The covid-19 virus is an RNA virus, and so on average mutates one or two bases on every reproduction.
2. When the virus kills its host, it also dies, since a dead host does not cough or breath.
3. Darwinian selection will then result in a less lethal virus over time, or the virus will not survive.
4. The July covid virus is not the same as the February or March virus.
So, why is this simple virology fact not discussed more. Today we hear about cases rather than deaths. Could it be that those in power and the media have an agenda to keep the level of fear high for reasons other than spreading the truth?
E
Brian writes:
Dear Vincent and team,
I’ve listened to some of your podcasts for a couple of years, and am grateful. You rock.
Recently I heard your team express doubts about aerosol transmission of Covid-19. Like the WHO, they pointed out large droplets comprise part of the total volume of expelled respiratory droplets, in sizes greater than 20 um. Virus presumably on the larger ones.
But evaporation time for droplets any of these sizes is very short, because they have an enormous surface area compared with their mass. For example, a 12 um droplet will take approximately 0.02 s to evaporate. A 25 um droplet will travel perhaps 5 cm before it shrinks to 5 um.
Humidity, temperature, mucin content of droplets, will all have an effect on evaporation rates. But virus on a larger droplet will soon enough be on a droplet nuclei, small enough for air resistance to take over.
So I assume you’re right, virus are on larger droplets. But those aerosols are dynamic and become flyers. Some references are below.
Brian Coyle
once an academic (soils, land tenure, West Africa) now inventor. Passion: evolution.
PS: Compartmentalized epidemiological models don’t include complex households, where most transmission occurs. These may have people of different ages, health conditions, circulation patterns, protective behavior. Within the housing area they can interact in different ways. Here’s the thing: it’s probable that within-household behavior is a more significant transmission variable than outside-household activity. People interact for longer periods, in smaller areas, in them. This has significant epidemiological effects. I would guess that if household risk is greater than circulation risk, backwards bifurcation results.
PPS: Somebody wrote in worrying about elbow bumping, wondering if virus were mobile. Mobility no, but consider this: people are told to sneeze and cough into the crook of their arm. Last I checked, elbows are on the flip side. That does seem a bit too close for comfort.
Beggs, Clive. (2003). The Airborne Transmission of Infection in Hospital Buildings: Fact or Fiction?. Indoor and Built Environment. 12. 1-10. 10.1177/1420326X03012001002.
Wells, W. F., Airborne Contagion and Air Hygiene; an Ecological Study of Droplet Infections. Cambridge,. Mass., Harvard University Press, 1955
Juan writes:
Dear Twiv,
It’s 33ºC degrees here in Milan, Italy. Around 91 F I believe. We passed the peak of covid a few months ago although the number of daily cases are still near the ~100s. Many of these, however, are only found after serology tests done to (seemingly) healthy individuals which after finding they have antibodies are tested and turn out to be PCR positive.
Regarding these “weakly positive” individuals (as the authorities here are calling them) the head of one of the most important hospitals of Milan has claimed the virus is now “less powerful” (in English:
https://www.cnbc.com/2020/06/02/claim-coronavirus-no-longer-exists-provokes-controversy.html).
The claims look intentionally controversial I don’t give them much importance, but the following related question has come to mind:
I’ve heard several times that the threshold (or whether there is one) for infection with SARS-CoV2 (and indeed most viruses) is not known. For the sake of the question, let’s assume such a perfect threshold exists.
To me that means that below the threshold we get virus particles in our bodies but do not get infected. How would these particles be cleared in a naive individual? Does the body learn to eliminate them? Can a person gain a certain degree of immunity (of any kind) by being exposed to very small quantities of infectious virus? Can this be the way the covid becomes another “common cold”?
I guess this impossible to study in humans, humans right and all, but I wonder whether the answer to these questions are known (maybe for other viruses) in animal models.
I am “just” a particle physicist and my knowledge of anything bigger than an atom is very limited. Now thanks to you I am learning to appreciate how stupidly exciting these non-alive creatures are. The non-covid episodes are discovering me so many new ways I can die, but also so many exciting new things that I can’t stop listening. Thanks!
Note: I guess you guys already have access to this kind of data, but I wanted to point out the Italian epicentro website, which collect the official data since the beginning of the outbreak:
https://www.epicentro.iss.it/en/coronavirus/sars-cov-2-dashboard
Thank you very much for all your work!
Juan
John writes:
Hello TWIV crew. I am a geriatric doctor with an long standing running/biking habit. During those hours of zen, it occurred to me that the risks of SARS-cov-2 transmission/reception are mostly related to breathing! I have been holding my breath while passing others on the trail. One can stop breathing about 20 feet on approach, and resume 20 feet in passing. In my simplistic model, this assures adequate protection. Now this will not mitigate the ill feelings of others, and I have no objective evidence, but this helps me feel better.
Thanks for all you do
John Terry MD
Luis writes:
Dear Vincent, Rich and Kathy,
I am a recent, but now avid listener of Twiv. Your podcast is an island of wisdom, reliable information (and even entertainment) in a time of mounting uncertainty, ignorance and chaos.
I wanted to call your attention to the comment that was published in Lancet, along with the original paper on the Spanish SARS-CoV-2 seroprevalence. If you had seen it, you would have read “(…) In light of these findings, any proposed approach to achieve herd immunity through natural infection is not only highly unethical, but also unachievable.(…).” (attached). So the press was right on this one, and I was disappointed that you were so dismissive, when you did not see the accompanying comment. Also, the fact that someone was infected and recovered does not (at this point) guarantee that the same person cannot be again infected within months and perhaps suffer a much more serious form of the disease as you have just discussed in a previous episode (Twiv 635 with Daniel Griffin). I do not see how you get to herd immunity with unacceptable loss of lives! This does not even begin to count the long term effects of an infection by SARS-CoV-2. Time will tell what kind of chronic conditions will emerge…
To be clear, I am with the authors of the comment on this, as I think considering natural herd immunity can be achieved not only is ill informed but highly unethical, and has real life consequences! In addition, I am surprised by the argument that perhaps seroprevalence grossly underestimates true exposure to the virus. While I am convinced that cellular immunity is perhaps more important in this infection (the ones where cellular immunity controls viral replication quickly not only do better but develop lower antibody titers), I do not see that T cell responses occur without also mounting an antibody response. In fact, looking at T cell responses, CD4s are the ones that are invariably present on the exposed patients, and these are the type of T cell responses that correlate with an antibody response. On the other hand, a recent paper in Cell (attached) shows that among unexposed individuals, 40-60% (!) show SARS-CoV-2-reactive CD4+ T cells, which suggests cross-reactivity with “common cold” coronavirus, but which significance is unclear.
I look forward to more episodes! Best wishes from a sunny Lisbon and 25ºC. Luis.
Luís F. Ferreira Moita, M.D., Ph.D.
Innate Immunity and Inflammation Laboratory
Instituto Gulbenkian de Ciência
Portugal
Jon writes:
Dear Twivers,
I wholeheartedly agree with Prof Racaniello’s outburst about the CDC trying to kill us all with their recommendations against covid entry-testing of returning “IHE” students, faculty, and staff.
Maybe it is time to hold a listener contest for what the acronym CDC stands for. My entry will be “Center for Disease Contagiousness”.
-Jon
Eli writes:
Dear Drs. TWiV,
I am really glad I discovered your podcast a few months ago and hope to continue listening long after the current crisis is a historical footnote. I appreciate that your explanations are usually clear to non-scientists and especially that your expertise is combined with an admirable dose of “we don’t know”. I wish more people in public understood that an honest admission of ignorance BUILDS credibility.
I hope you don’t mind practical questions about how best to proceed in business. My spouse and I run a used bookstore and coffeehouse in the northwest corner of Washington State. (67F and sunny. We only occasionally get above 80 and at 85 the town mostly shuts down. Thankfully, air conditioning isn’t really a thing in these parts).
After a few months of being closed to the public, we opened our doors again last month. Our biggest issue now is how to buy used books from the public again. Our shelves are lighter than we like and there is an embarrassing number of holes in our stock. We’re also fielding no less than a dozen calls a day from folks who want to sell us books.
Our current plan, once we find available space near the shop, is to quarantine the books for 72 hours before processing them and another 72 before shelving them. Unfortunately, securing a space is proving difficult and we’re questioning whether those precautions are wise or necessary. And even if we have the space, that seemingly simple 6 day rotation is a logistical nightmare.
• We have great ventilation—We renovated the building a few years ago and invested in an air handling system that can exchange (not recirculate) the air in the shop every 90-120 minutes. It has been set to high since March. When customers are present the doors are open and the bathroom fan is always on.
• Masks are required of employees and customers and we insist that everyone don fresh gloves or use hand sanitizer as they enter the space. Bottles of hand sanitizer are scattered throughout the store and commonly touched surfaces are wiped down with alcohol or quaternary ammonia solution several times an hour.
• While plexiglass is awfully dear these days, our work-around has drawn many compliments (see attached photos).
• We limit customers in the store to about 25% of normal capacity. All coffee and food is for takeout only, we could legally allow a very limited amount of inside seating but decided that unless a customer can drink a latte through their mask, they must take it outside. Blessedly, no one has tried.
• Our staff is taking safety as seriously as we are and understand that if anyone feels ill at all they are not to come to work and will be paid for their shift anyway. We also check every employee’s temperature before they begin their shift.
• Until this week, we quarantined and disinfected all cash. My wife was going nuts with the bags of bills and we noticed that we were the ONLY place in town doing it. Still, anyone touching money is wearing gloves and no one who prepares food or drinks touches money.
So that’s the good stuff. But there is other stuff, largely out of our control, that worries us:
• Our small staff ranges in age from 21 to 75. We are confident that none of them are engaging in overtly irresponsible behavior but several are young, living with roommates, and falling in love. We’ve had to discreetly inquire about parts of our employees’ lives that should be none of our business. To our knowledge, none of our staff’s intimates have fallen ill but there have been cases of Covid in the same social circles they swim in. We fear it is just a matter of time before someone on the staff tests positive.
• We don’t have the same issues with close quarters that a lot of retailers and restaurants do, but 6 feet just isn’t possible much of the time. We are sanitizing computers between users and only my wife and I answer the phone, but there is no practical way to never miss a spot and never be only a couple feet apart.
• Maybe because we are a bookstore or maybe because we live in Lake Wobegon, our customers skew heavily to the right of the bell curve; we’ve been remarkably free from knuckleheads. But the nature of a bookstore means that people are going to browse, pausing in front of shelves, touching multiple books, generating an invisible cloud of whatever their bodies are shedding despite the mask. Even if a mask blocks 90% of viruses, it still means that 10 minutes in one spot is going to leave the same cloud that someone would leave after one minute without a face covering…Right?
• We’re proud of our Governor’s response. But shutting down once nearly broke us. If we close again because the State orders it or because someone on staff gets sick, we might not be able to open again. To say the least, I am unimpressed with folks who are blasé about masks and other precautions.
So back to the original question: How do we buy used books? Our operating assumption is that every book someone tries to sell us was sneezed on by someone with a full blown case of covid ten minutes earlier. Of course that isn’t true, but is it a reasonable assumption to build protocols on?
Besides quarantining them, we’ve toyed with bringing out the ozone box we sometimes use to deodorize stinky books. But using that comes with its own set of safety and logistical issues. It seems surface transmission is rare but not impossible. Paper doesn’t seem to hold live virus very long but most book covers these days have a thin layer of plastic. We’ve always wiped down many books with sanitizing wipes anyway, extending that habit to every book is doable but expensive at scale.
On one hand, I feel like we are already doing so much that quarantining books is like installing seat belts on a train.
On the other hand, because of the nature of our business and the inherent risks of having employees who live in the world, it seems like anything beyond the basics is like putting mosquito screens in the windows of a house with no roof.
I’m really bad at quantifying risk. What can we do that is really helpful and what is just theater? What are we missing? What would you do?
Thanks for all ya’ll do!