
Anthony writes:
Oh no, it’s hookworms! Grab the ivermectin quick!
Regarding the last case about the eye amoeba – I had forgot to share the paper pointing the finger at Vahlkampfia:
https://pubmed.ncbi.nlm.nih.gov/12799148/
– Anthony
Alexander writes:
Dear TWiPsters,
the woman who returned from Puerto Rico probably suffers from an early stage infection with hookworm, most commonly either A. duodenale or N. americanus. This geohelminth is transmitted via soil when the L3 larvae come in direct contact with the skin and manage to penetrate it. This leads to intense itching and these serpiginous lines. Later stages of the infection can cause gastrointestinal problems and anemia, which can be severe and sometimes requires transfusions.
Prevention is achieved by wearing closed shoes in areas where hookworms are endemic, building toilets with adequate plumbing or at least latrines with a depth of over 6 feet and deworming programs. The therapeutic agent of choice is albendazole.
Interesting fact: The complex cycle of infection of this group of parasites was discovered at the Gotthard tunnel construction site in Switzerland during the late 19th century. An epidemic of diarrheal illness and anemia was linked to the workers defecating in the tunnel and walking about in worn-out shoes with holes in them.
All the best and take care,
Alexander
from Vienna, Austria
Kevin writes:
Dear Magnanimous Drs.,
My case guess for TWiP 194 is cutaneous larva migrans caused by Ancylostoma braziliense. I had doubts because many sites describing soil transmitted helminths do not mention A. braziliense, but perhaps this is simply an oversight on their part.
Warm regards,
Kevin H
Adil writes:
Elevated eosinophils, Puerto Rico and lower extremity lesions make me think hookworm. You mentioned beach walks and someone also asking about dogs in passing. You said it’s an easy case so I’m confident enough. By time of reading this may count as my first guess as an MD.
Adil
Joe writes:
It’s in the mid 60’s with low humidity, sunny with little wind in Seattle as I write this.
After years of enjoying TWIP from its onset listening to periodic descriptions of various and sometimes shocking diseases described in attractive New York accents, I am finally moved to enter my prognosis to the disease described in TWIP 194, the lady who visits the sandy beaches in Puerto Rico who developed itchy, red patches on her feet. My prognosis is not based on education and training but on personal experience (“The kind that makes you sick.”)
I was raised in New York City during the 1940’s to early 1950’s. At that time, a scourge attacked New Yorkers, particularly school age children. The rapidly spreading disease affected mostly the scalp of children, including myself causing patches of baldness and red markings. The outbreak of an unknown disease alarmed parents, teachers and New York doctors who did not know what was causing the ugly patches on children. Apparently, at that time tropical skin diseases were not part of standard training for New York physicians.
While the cause of our disease was unknown by NY doctors, many affected children were treated by applying a variety of common substances such as vinegar, dilute Clorox baths, talcum powder and the like. I still remember my parents shaving my head to baldness and trying ultra-violet treatment by placing a purple light-bulb on my head for hours. But nothing seemed to work. That is until it was discovered by a Russian doctor working for the City Department of Health that high-intensity x-ray treatment of the scalp successfully treated the disease.
So, the NY Dept of health arranged to have all school-age children line up in the halls of the Bellevue Hospital on the East Side of Manhattan to take their turn to have their scalp x-rayed. The procedure was quick. First one side of the scalp was scanned with high-powered x-rays then the other side of the scalp was scanned. One child after another for days to months were treated and the scourge finally went away. It was a total success. So they thought.
In the mid 1970’s and in my 30’s, I noticed some bumps on the back of my scalp under the hair-line. The bumps were itchy and grew fairly rapidly. A visit with a demonologist confirmed squamous cell carcinoma, skin cancer appearing on a very unusual place of the body, under the hair which is rarely exposed to the sun.
I was not alone. About the same time, I learned that many of us developed skin cancer under the hair line, along the center-line region of the scalp. Apparently, as our heads were x-rayed the area along the center of the scalp received a double dose of high-intensity X-rays.
What caused us to be x-rayed is the same parasite that the lady who frequented the beaches of Puerto Rico suffered, a fungal disease commonly called ring-worm. I don’t believe x-rays are still used to treat it.
Not being a member of the medical profession, I will not suggest a prescription of antifungal creams which Dr. Google suggests. I don’t want to be responsible for problems that may develop twenty to thirty years later.
Joe
Alex writes:
The answer is Cutaneous larva migrans! (Which is “caused by the larvae of various nematode parasites of the hookworm family (Ancylostomatidae)”)
I just googled the word serpiginous (which I’ve never heard before) and the first image result gave the answer. The Wikipedia article mentions that “Hookworm eggs are shed in the infected dog (or other animal) feces to the ground and beach sand”.
I’m happy that Daniel said the lines were migrating because up to that point I was certain the question was intentionally easy to throw people off the trail.
This is the 1st case I’ve ever guessed! I only started listening to you recently and this is lots of fun!
– Alex, from Israel
Owain writes:
Dear TWIP,
Thanks to Vincent for artfully making sure my email got read on TWIP 194! I laughed out loud when listening to how I nearly failed to make the cut! To make up for that and to ensure it doesn’t happen again, I’m submitting this much more promptly.
My guess this time is CLM – cutaneous larva migrans. The most likely cause is a dog hookworm, Ancylostoma caninum or braziliense. Less likely differentials would be human hookworms or Strongyloides which are making their way to the bloodstream having percutaneously entered their host.
While this submission might not win me a textbook, my increased speed at sending this in makes me feel like a winner regardless… still trying for the book though!
All the best,
Owain
Byron writes:
Dear TWIP hosts,
I was listening to TWIP while driving my son to his tennis practice, and upon hearing Dr. Griffin’s case. I responded, ” Oh, I know about that one”. I actually could not remember the exact kind, but the picture of the foot with serpiginous lesions immediately came to mind. My son, then turned his head (away from his phone, I might add) and look at me saying ” how do you know what?” The look on his face, priceless…
well, my guess is this is a nematode infection causing cutaneous larva migrans.(LCM) from dog and cat hookworms Acylostoma braziliense and Uncinaria stenocephala. I hope I am right this time, Thank you for everything you do! It is 61F, 16C and cloudy in Naperville, Illinois.
Byron
Antoinette writes:
Hello, I am a visual artist from Melbourne, Australia (currently 24 degrees C).
I actually haven’t done any Biology since high school, but my curiosity grew over the last year after I found Vincent’s virology lectures on YouTube. Now I’m hooked on all things microbe.tv and look forward to all of the “this week in…” on the channel. I am also half way through Brianne Barker’s immunology online lectures (I may be in over my head).
My initial guess was Scabies but after a little research based on the clues – Puerto Rico, raised red lines and dogs on the beach – I think it is Cutaneous larva migrans caused by larvae of hookworms.
But as I haven’t taken a YouTube course on parasites yet, I could be completely wrong! Any recommendations on online lecture series would be appreciated.
Stay safe. Keep up the fabulous work.
From all the way down under,
Antoinette
Peter writes:
Greeting to the luminaries of the TWIP-o-verse
The woman in TWIP 194 who visited a beach in Puerto Rico is probably affected by Ancylostoma braziliense, the dog (or cat) hookworm. The serpiginous lesions are a tell-tale sign [1]. Eosinophilia can also be present as it is in this case [2] and while it may also be absent, hookworms are rarely associated with a form of pulmonary eosinophilia called Loeffler’s syndrome.
If I am correct, this is the same affliction as was covered in TWIPs 123 and 150. Researching this disease I was struck at how – as is typical for medical photographs – the imagery was all of red or brown lesions on pale skin. What does CLM look like on darker skin tones? I include an image from Brazil [3]. Notice how the lesion is much less visible.

And in this image from India [4] one can see how the lesion appears light and almost shiny:

As the issue of racism in medicine is currently getting some much needed attention, I think it is useful to highlight the need to include a diversity of images in the descriptions of disease symptoms.
Thank you once again for your efforts,
Peter
from a somewhat chilly (16 C) Cape Town. Still no COVID-19 vaccines in sight here, although we are told the long awaited vaccination of elderly and vulnerable groups should start in mid-May and apparently 325,260 doses of Pfizer vaccine are arriving in South Africa tonight.
1. Parasitic Diseases 7th edition, page 300
2. Heukelbach et al Epidemiological and clinical characteristics of hookworm-related cutaneous larva migrans, The Lancet Infectious Diseases Volume 8, Issue 5, May 2008, Pages 302-309
3. Schuster et al Life Quality Impairment Caused by Hookworm-Related Cutaneous Larva Migrans in Resource-Poor Communities in Manaus, Brazil, PLOS Neglected Tropical Diseases November 8, 2011
4. Aroor et al Cutaneous creeping eruption in a child Our Dermatology Online 2016.1-34
Trudy writes:
Dear TWiPers,
Here I am, showing up for the easy ones. The lady who returned from Puerto Rico has a case of cutaneous larva migrans, caused by nematode parasites of the hookworm family.
Thanks for the continued edutainment!
Best Regards,
Trudy
Annie writes:
Hello,
I hope you’re all doing well! I’m a first-time listener of the TWi series and thought I would give the case study a shot. It sounds like the woman is suffering from cutaneous larva migrans, which occurs when hookworm larvae penetrate the skin. It’s not uncommon for this to happen at beaches when people are walking barefoot, especially on beaches where dogs are allowed. This diagnosis is also supported by the elevated eosinophil levels, which are a common feature of helminth infections.
Best,
Annie (a PhD student)
Neil writes:
Greetings from Ireland, where it’s 5 Celsius, wet and windy 365 days a year. However, the work you do at TWIP virtual studios is the light of our lives. Particularly Dickson, who we would love to welcome to Dublin for innumerable pints of Guinness as soon as we’re released from this travel ban.
In the meantime, thank you to Daniel for another wonderful case. It is of course cutaneous larva migrans. This is principally caused by dog and cat hookworms. Of these, I would favour Ancylostoma braziliense in this case, given the mention of dogs in the vignette. The L3 larvae of these nematodes can survive in sandy, moist soil for days and are particularly common on Caribbean and south East Asian beaches. The clinical phenomenon described is what is commonly known as the “creeping eruption”, typically apparent after an incubation period of approximately a week. Diagnosis can be confidently made on clinical grounds, given the distinctive nature of this presentation. Although as referenced, where bloods are taken they do typically show an eosinophilia or elevated IgE. Treatment consists of anti-helminthic therapy – single dose ivermectin representing a simple and effective regimen.
Go raibh míle maith agaibh.
Neil
Joel and Bronwyn write:
G’day Twip-aroos
I’m writing from Bundaberg, Australia; home of the eponymous ginger beer.
I believe the woman who enjoys long walks on the beach has a case of cutaneous larva migrans (CLM). The pictures that you described show the “creeping eruption.” While this specific sign was described in Dickson’s lecture on hookworms as a manifestation of Ancylostoma caninum, Parasitic Diseases (6th edition) indicates that this particular parasite is more associated with eosinophilic enteritis here in Queensland! A more appropriate guess considering the geography would be Ancylostoma brazilienses, although a variety of hookworms can still present as CLM. Whatever the culprit, a prescription of albendazole is likely adequate first line treatment along with preventative measures: either footwear for her sandy strolls or limiting them to biped exclusive beaches.
Thank you for your podcasts which manage to be both educational and entertaining. We always look forward to the next one.
-Joel and Bronwyn
Martha writes:
Dear TWiPs team: The case presented at the end of episode 194 jarred loose some memories. I believe I have personal experience with the parasite in question.
About 40 years ago I had just relocated from Connecticut to south Florida. I had not yet developed the habit of gardening with gloves. Perhaps it will not surprise you to learn that I developed a very itchy rash on my hands. I had relatively few lesions which seemed to increase in length in a wandering fashion. I was told by the locals that the rash was called “creeping eruption” and was caused by gardening. My PCP told me it was cutaneous larva migrans, caused by cat or dog hookworms. The larva lacked the enzyme to break through the dermis and would eventually die. Since I had only a few lesions the treatment of choice was freezing with liquid nitrogen. This was done by freezing a point just ahead of the advancing line. I later found that with salt and the corner of an ice cube I could generate cold sufficient to euthanize new larval lesions.
I did look up the names of the most likely actors in this: Ancylostoma canium and A. brazileinse. In these more enlightened times the treatment is apparently with thiabendazole or albendazole. I no longer have this issue since I have returned to New England and I garden wearing nitrile gloves under my elbow length leather gauntlets.
Best wishes to you all,
Martha
The Parasitology Club at the University of Central Lancashire writes:
Dear TWIP Professors,
Greetings from The University of Central Lancashire in Northwest of the United Kingdom, on this extraordinary sunny day, but cold as the temperature outside is 6 Celsius or 42.8 F as we write to the case 194. It is always awesome to listen to exciting new cases we all look forward to listening to your amazing Podcasts.
Lancashire has some amazing history, a small town within Lancashire called Burnley is a historic market town with amazing surrounding countryside called the Pennines (et, al Burnley, Lancashire | Discover Britain’s Towns, 2021.) We have provided a link of our university’s history starting from 1828 please find the link at the bottom of our letter.
The serpigenous eruptions appear to resemble the descriptions of cutaneous larva migrans (CLM). The culprit is one of the hookworm species and most likely Ancylostoma brazilliense which has a wide geographic distribution but is noted for infections associated with walking barefoot on soil or beaches in Southern and South America and the Caribbean. The rhabditiform larvae of the helminth can penetrate the skin and migrate along the dermal layers of the skin causing intense itching and redness.
Diagnosis is normally clinical in this dermal infection. Shimogawara and colleagues (2013) reported increased peripheral eosinophila correlated with disease severity in CLM and which decreased following treatment with ivermectin.
Neal Vickers
All the best, safe wellness from The Parasitology club at The University of Central Lancashire.
Shimogawara R, Hata N, Schuster A, Lesshafft H, Guedes de Oliveira S, Ignatius R, Akao N, Ohta N, Feldmeier H. Hookworm-related cutaneous larva migrans in patients living in an endemic community in Brazil: immunological patterns before and after ivermectin treatment. Eur J Microbiol Immunol (Bp). 2013 Dec;3(4):258-66. doi: 10.1556/EuJMI.3.2013.4.4. Epub 2013 Nov 21. PMID: 24294495; PMCID: PMC3838541.
www.uclan.ac.uk
https://www.uclan.ac.uk/about-us/history
Caton writes:
Greetings all Ye of the TWiP persuasion:
I suspect the woman who visited the local beaches in Puerto Rico walked through the sand barefoot and got infected with Ancylostoma braziliense, a hookworm that had been previously deposited by a fellow beach lover’s canine companion. Seeing as the woman was about 40 years old, she likely carried in her own beach chair, thus saving her from finding the dreaded cutaneous larva migrans on other unmentionable locations.
Reading about hookworm, I discovered a new vocabulary word, “PRURITIC”. I had to look it up as I am not a doctor, I am just a lady farmer. This is when I questioned certainty of my amateur diagnosis. I went back to Daniel’s telling of the case story on TWiP 194. He states that the woman “noticed” some slow moving raised red lines on her feet and took pictures of them as they grew over time. Now, Daniel, didn’t she “notice” that those raised red serpiginous lines were incredibly itchy? Also, I wonder: would the high level of eosinophils contribute to the itchiness of the pruritus?
I sure hope I am on the correct serpiginous track.
Caton
S&C Nelson Farm, Grass-fed Beef
Iron River, MI 49935 It’s Michigan—not Missouri
Dhruti writes:
Dear TWIP Team,
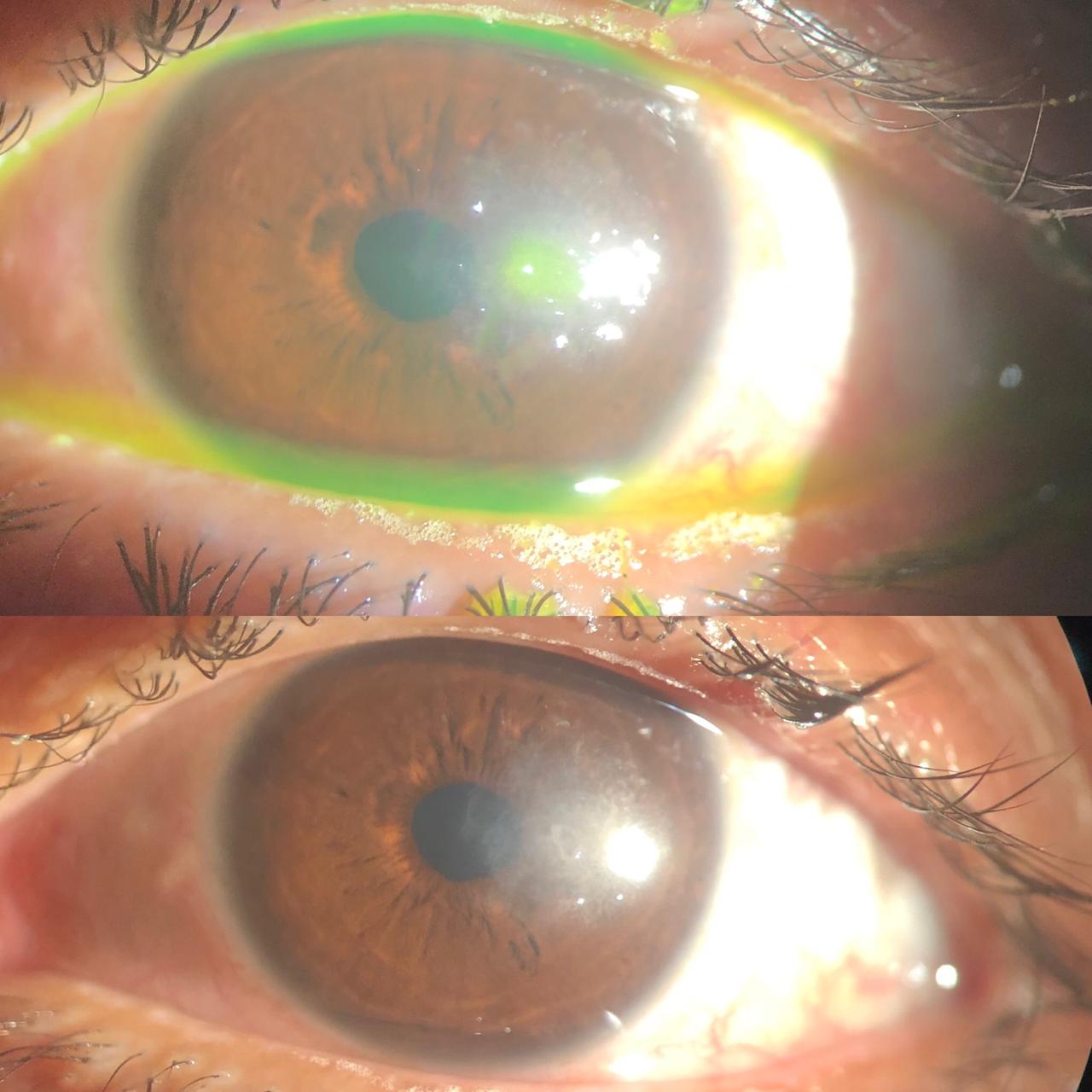
My answer for twip 193 – 50 year old gentlemen with vision problems and painful eye possibly is suffering from Acanthamoeba Keratitis. The history in this case is a very typical one – contact lens wearer, washing lenses with tap water. Last month we had a similar case, a female in her thirties- contact lens wearer, poor maintenance of contact lens cover and solution. We got corneal scrapings which we stained with Giemsa stain and we were able to see the trophozoites. It was also associated with Pseudomonas infection. We also got hold of her contact lens cover and solution where we grew Pseudomonas Aeruginosa. I tried to do the lawn culture of E. Coli on a nutrition deficient agar and added lens solution on it. Ideally you see tracks of Acanthamoeba. I saw the track but was unable to see the parasite under Microscope. I hope Dr Despommier can help me to improve my technique.
I have attached photos of
1) corneal defect left with the infection
2) trophozoite on Giemsa stain
For Twip 194
This morning while I was commuting I was listening to a Parasite lecture on Hook worm (Parasite without borders) and while returning I listened to Twip 194. So my guess is a bit biased. A mid-forties lady returning from Puerto Rico was possibly suffering from Ancylostoma Caninum. Treatment will be thiabendazole ointment.
PS – Today we also received a CSF sample from a patient and I have attached two videos of that sample. We are querying Naegleria Fowleri which is distant cousin of Acanthamoeba (free living parasite, mostly infections are associated with untreated water). If Dr Griffin and Dr Despommier can help with the diagnosis that will be helpful.
Thanks for all the education
Dr Dhruti Sheth
M.B.B.S. , 1st year DNB Microbiology,
Breach Candy Hospital
Mumbai
Katy-Jane writes:
Hi all,
71 degrees and humid here in north central Wisconsin. I got the garden weeded and started planting yesterday.
Great to hear Christina Naula back on last month’s episode! There are plenty of parasites that can be contracted by playing on beaches, such as Toxocara canis and human hookworms, Necatur americanus, but these tend to cause symptoms other than itchy feet with serpiginous trails. My guess for our case study is cutaneous larva migrans caused by the larvae of Ancylostoma braziliense, a hookworm carried by dogs and cats. There are also other dog and cat hookworms that can cause this infection, but from a quick Google search, this species is the most likely culprit.
Thanks again for another great episode!
Katy-Jane Shanak
Adjunct Faculty in Veterinary & Dairy Sciences
Northcentral Technical College
Wausau, WI
James writes:
Dear TWIP-
I have really enjoyed the show and even got my lab into some of the guessing over the last couple of episodes. We study alpha herpes viruses. As I’m writing this email sitting on a beach wondering if I’ve stepped on a parasite myself, my guess to the case of the 40 year old woman that frequents Puerto Rico is cutaneous larva migrans, Ancylostoma braziliense. Keep up the great shows and work! Thanks James!
David writes:
Dear professors,
For the first time in over a year, I finally have caught up with TWiP – that with the virology podcasts bringing us tidal waves of scientific backgrounds for SARS COV2. It is so impressive how much each of you manages to do in the midst of a pandemic – podcasts aside, it makes my own achievements look rather small and all three of you are a constant source of inspiration.
When I listened to the last episode, I couldn’t help but smiling. Dogs and beaches, it seems a fatal coincidence. My guess is Cutaneous Larva Migrans caused by Ancylostoma braziliense, or as PD 6th edition puts it:
L3 larvae … are especially common on beaches in … Puerto Rico, where dogs and cats are permitted to wander the beaches and freely defecate.
Pure poetry. Hope I’m right and in time with my submission.
For your reading pleasure…
After she got her diploma
She loved Puerto Rico’s aroma
She went to the beach
The dogs off its leash
Her foot now shows ancylostoma
Yours truly,
David, in an ever sunny Nicaragua
Elise writes:
Dear TWiP Trifecta (and any guests),
I do hope this finds you all well. It is sunny and 72 degrees F (22 degrees C) here in Lower Manhattan. I’m very sorry to have missed my chance to submit a diagnostic guess for TWiP 193. The last few weeks have gotten suddenly busy. (I’m pleased to say that one of the things that has kept me running around has been the project of getting my family vaccinated— one family member had to be hauled all the way out to Staten Island — TWICE — for his because I was so eager to get him vaccinated as soon as possible.)
My guess for the vacationer in Puerto Rico is that she came back from her holiday with Cutaneous Larva Migrans, taking their own vacation to the United States. It is not at all uncommon for animals of various sorts to deposit these hookworm larva on beaches (or in sandboxes) and then exposure through barefoot walking on the hookwormy sand allows for infection. The patient’s symptoms are pretty classic for the infection. The CDC says that these infections are usually self-limiting (the migrating larvae usually die within six weeks), but treatment with Albendazole or even Ivermectin is very effective.
Will the patient need to treat her dogs for hookworm now after this vacation? I know that it is generally protocol for veterinarians to recommend always giving dogs medication to guard against heartworm, but does hookworm need to be treated in a different way?
Thank you so much as always for everything you do and many best wishes,
Elise (in Lower Manhattan)