
Anthony writes:
Likely an amebic infection of the eye caused by either Acanthamoeba or Vahlkampfia since these ameba are oddly able to live in saltwater!
Anthony S.
Allan writes:
Greetings TWIP friends,
Weather here in Kona is 80ºF/27ºC, 70% humidity and partly cloudy.
I believe your patient is most likely suffering from Acanthamoeba Keratitis caused by the protozoan Acanthamoeba castellanii.
While there are many microbes that can infect the eye and cause the described signs and symptoms, the primary one associated with untreated water and contact lens use is Acanthamoeba castellanii.
While identification through PCR is possible, definitive diagnosis usually still depends on seeing the ameba in tears or scrapings such as with a rapid Field’s stain.
Treatment has historically been difficult and rather than describing old methods I look forward hearing more promising approaches from Daniel et all.
Thank you again for your wonderful podcasts.
Allan
Allan Robbins, DIH, MPH
University of the Nations
Hawaii
James writes:
Hello TWIPPERS,
I am a big fan of all of the This Week In podcasts, but have never sent in a case guess, but decided to do so for the parasitic eye infection presented in episode 193. I’m a commercial lender with no formal medical training, but I know you’ll be kind.
The patient presented with irritation and edema of the left eye, accompanied by decreased visual accuity and erosions of the cornea. Of note, the patient is a soft contact lens wearer and lives on a rural property with its own well and septic tank.
My guess is that the gentleman has a case of Acanthamoeba Keratitis, caused by the protozoa Acanthamoeba, which is a very common organism found in soil and freshwater environments worldwide. Acanthamoeba is transmitted through direct contact between the parasite and the cornea of the eye—and poor contact lens care is a major risk factor for developing acanthamoebiasis.
I believe the most likely source of infection is contaminated well water being used to clean and store the patient’s contact lenses. In 2016, Jennifer R. Cope MD, et. al. published a case-control investigation of two multi-state AK outbreaks among rigid contact lens wearers and found that even using tap water to store RGP lenses and top off solution in the lens case were risky behaviors. My research also uncovered a 2006 case, published in the Canadian Journal of Infectious Diseases and Medical Microbiology, of AK in a healthy 14-year old soft lens wearer, where “an epidemiological link was established between the patient’s isolate and well water from the home using molecular methods.” That paper also cites two other cases of AK caused by contaminated well water.
Thanks for keeping me entertained and educated!
James
Caroline writes:
Hi!
For this case, I think the patient was infected with an Acanthamoeba, causing an acanthamoeba keratitis.
I found this article, that lists a good number of known fungal and parasitic eye disease, very helpful:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC88956/
Acanthamoeba can be found in improperly treated water supplies and contact lens solution, either of which could have been the origin of the disease in this case since he doesn’t treat his well water and he uses contact lenses.
Its symptoms include eye pain, decreased vision, redness and discharge, which the patient had.
The corneal scrapings can be used to view trophozoites and cysts in stained preparations, to confirm this diagnosis.
Treatment is difficult. Different medicinal regimens exist, involving antifungals, antibiotics, etc. However, apparently these often don’t work and the patient may need surgical intervention. Even with surgery, if cysts are still present, the patient may continue to suffer from recurrent infections.
Thanks again and stay safe!!
Caroline
Laura writes:
Warm spring greetings to everybody at TWiP!
I really liked ophthalmology when I was in medical school, but more on a theoretical level and I was pretty good at diagnosing photographs. However, when watching actual examinations or procedures, my eyes would tear up so bad, I couldn’t actually see much.
My diagnosis for this case is amebic keratitis caused by Acanthamoeba spp. The organisms have no vector, they live in bodies of water and soil, where they feed on bacteria and debris, but have also been found in tap water and air conditioners. They have to come in direct contact with microabrasions on the cornea to be able to infect it.
These protozoa cause a subacute or chronic keratitis (inflammation of the cornea) associated with contact lenses (in 80% of cases) or corneal trauma.
It is interesting that some bacteria, fungi and other protozoans can survive inside Acanthamoeba in a possibly symbiotic relationship, increasing pathogenicity and complicating or hindering treatment.
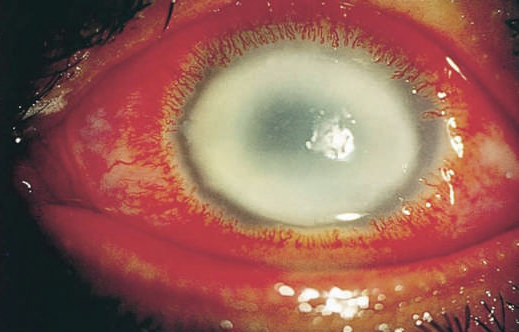
The keratitis presents days after infection with pain, photophobia, tearing, dendritic ulcers and a characteristic ring infiltrate:
The differential diagnosis would include viral (most often herpetic), bacterial and fungal keratitis.
The definitive diagnosis is established via corneal scraping or biopsy with wet mounts, culture, histopathology or PCR, or more recently, in vivo confocal microscopy. The contact lenses and contact lens solutions can also be cultured.
Treatment options are topical chlorhexidine, polyhexamethylene biguanide or voriconazole, to which oral therapy can be added with azoles or miltefosine. Medical treatment is 80-90% effective and surgery is sometimes required.
Prevention measures include changing the cleaning solution every night, only using commercial solutions and not homemade, although cases tied to some commercial solutions have also occurred, letting the contact lens case to air dry thoroughly every day and changing it frequently. Contact lens wearers should never go swimming or showering with their contacts on.
Thank you for this interesting case!
Patiently waiting for the next episode
Laura
Byron writes:
Distinguished TWIP hosts,
Have to say, this is a very interesting case! My guess was Giardiasis. Although it is commonly known for GI symptoms, I do find some cases of ocular involvement. Here is the link
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3806574/
Thanks for all the work, and all the interesting cases! My background is not related to medical, but found this immensely intriguing. Thank you!
Byron
Alexander writes:
Dear Professors,
the differential for a middle-aged man with unilateral keratitis is quite broad; Aside from non-infectious etiologies such as direct trauma, lagophthalmos, often as a consequence of facial nerve palsy, or foreign bodies stuck under the eyelid, many different pathogens should be considered.
Since viral conjunctivitis is typically bilateral and fungal keratitis rarely occurs in immunocompetent individuals, bacteria and protozoans should be a the top of the list. A notable exception is herpes simplex keratitis, which can also be considered here and can usually be identified by the classically dendritic appearance of the corneal ulcers.
The most common bacteria that cause keratitis in healthy subjects are Staph. aureus and Pseudomonas aeruginosa. In patients using contact lenses, Pseudomonas can cause corneal ulcers that require immediate therapy with iv and topical antibiotics. Rarer causes include Leptospirosis, Melioidosis and Trachoma, which don’t really fit the history here.
The classical protozoan to colonize contact lenses if improper cleaning solutions are used is Acanthamoeba spp. Others are T. gondii or Giardia, which are less typical.
I believe this gentleman is in for a long course of topical combination therapy to kill off all his acanthamoebic friends and complementary bottle of sterile contact lense cleaning solution, or even simpler, a pair of glasses.
Thank you for the interesting case, take care!
Alexander
Vienna, Austria
Andrew writes:
Kia ora from Pongaora,
Weather: the La Niña has ended and we are returning to normal, yay!
Covid: The New Zealander of the Year has been voted for and it is a microbiologist named Siouxsie Wiles. She was, and still is, the most prominent science-communicator engaged in educating the public on SARS-CoV-2 and the pandemic in general.
https://en.wikipedia.org/wiki/Siouxsie_Wiles
Book: not won yet but did Daniel mention version 8?
My guess for the man with unilateral eye pain is:
Acanthamoeba keratitis caused by water contaminated with the microbes being used to clean his contact lenses. PD7 notes that the increase in contact lenses use is leading to more cases and now that they are being used for purely cosmetic reasons, I suppose that we will see even more cases in the future unless education in lens hygiene is also increased.
Nā,
Andrew
Martha writes:
Dear TWIPsters: I will try to be brief since I’m sure you will have many responses to this case. I do want to express my enjoyment of all the TWI podcasts. I plan my walks based on the program’s length. For Dr. Griffin’s updates I do a short loop at a brisk pace, while for the twice weekly TWIVs I can do a long leisurely stroll. TWIP falls in the middle, I try to plan to end the walk so I can jot down the case notes. So thank you for all you do. And its eyeball parasites again.
Interestingly, I happened to stumble upon this parasite as I was looking at images of infected eyes trying to find something that would be small enough to fit in the anterior chamber of the eye, but large enough to block the pupil. Acanthamoeba keratitis was not a suspect in that case, but swam to the top of the list this time. Giardia always comes to mind when well water is mentioned, and they can infect the eye, however they cause a retinal problem. I’m sticking with the amoeba since all the clues point in that direction: soft contact lense use, eye pain and visual changes, corneal scraping for diagnosis. Using that pure well water to wash the lenses was perhaps the source.
All the best to you all
Martha
Erika writes:
Hi TWiP,
Greetings from Toronto, where it’s 10°C and cloudy.
We are currently under a stay at home order in our third wave of the pandemic, so I can’t thank you enough for the company of your friendly voices. It’s thanks to this podcast, and TWiV, for rekindling my interest in science. I’m now working towards going back to school for pharmacy, after dropping out of engineering school eight years ago.
I always look forward to a new case study, so here goes my guess for the most recent one: Acanthamoeba keratitis.
Still hoping for a book,
Erika
Katy-Jane writes:
Dear all,
I remember listening to one of the earliest episodes of TWiP a few years ago where Dickson stated that you should never store your contact lenses in water…and “eye” have never done it since! This case reminded me of that episode, and Daniel’s avoidance of the question as to whether or not the patient was washing his contact lenses in well water supports my line of thought. So my guess is Acanthamoeba castellanii, causing Acanthamoeba keratitis.
38 degrees F and windy in north central Wisconsin, but the avian spring visitors are trickling in.
Thanks for all that you do.
Katy-Jane Shanak
Adjunct Faculty in Veterinary & Dairy Sciences
Northcentral Technical College
Wausau, WI
Caton writes:
Hello fellow TWIPers and TWIPies:
On the case of the aching eyeball, could it be the rare, vision-threatening condition of Acanthamoeba Keratitis? I checked my work with TWIP 39, and “I Encyst” this is the correct answer.
While I am not a doctor (I am just a LADY farmer), I assume that all the juicy details of this nasty eye condition will have been thoroughly discussed by everyone already. However, I have to say that the thing that strikes me about this particular organism is its “rarity,” or, rather, its rarity in causing disease. Acanthamoeba is actually quite common and most everyone has been exposed to it.
But, for the immune compromised, there is reason for further concern. Acanthamoeba can also causes disseminated infection by entering the skin through a cut, wound, or through the nostrils. Once inside the body, the amoebas travel through the bloodstream to other parts of the body, especially the lungs, brain, and spinal cord, causing the deadly Granulomatous Amebic Encephalitis. It is interesting to note that, according to the CDC, there have been no documented cases of Acanthamoeba spreading from the eye to other parts of the body.
While I enjoy participating in TWIP case studies, I have not coveted the winning the prize. However, while listening to TWIP 39, I have come to realize that I WANT THAT BOOK, so please, please, pretty please pick my number.
Caton Gauthier-Nelson
S&C Nelson Farm, Grass-fed Beef
Iron River, MI
Owain writes:
Dear TWIP,
I hope I’m not too late this month! Somehow I always think I’ll have plenty of time to submit a guess, but that often leads me to leave it to the last minute! A terrible habit…
My guess for this case is Acanthamoeba keratitis – he probably got it either from swimming with his contacts in, or the water from the well getting onto his contacts somehow! The horrible-sounding “corneal scraping” diagnostic procedure always makes me shudder..!
Keep the podcasts coming!
All the best,
Owain