
Eric writes:
Greetings!
Thank you for your fantastic flora of podcasts and online lectures. There is so much to learn and you are such pleasant educators.
Since Daniel said this was an easy case, I thought I’d give it a go.
My guess is that the poor teenager had been swimming among parasitic flatworms (Schistosoma Haematobium) and contracted Urogenital Schistosomiasis (also known as snail fever or Bilharzia).
Treatment is a short-course of Praziquantel.
Fascinating little worms. 🙂 Don’t go swimming with snails in other people’s pee.
I humbly bow to your knowledge and expertise and your healthy approach to science.
Linköping, Sweden. +2C, a light snowfall (with a Class 3 Warning of severe snowstorms for the night)
// Eric, just a curious listener
P.S.
I managed to find this rather amusing pearl on the web:
https://journals.lww.com/epidem/fulltext/2013/07000/case_fatality__rate,_ratio,_or_risk_.23.aspx
From now on, I am a Risk person.
David writes:
Hello Team TWiP,
Wonderful episode as always. Thanks for continuing to provide the listeners with your insights into the world of parasites, parasitic diseases, and scientific research into the same. The show is an intellectual diversion from the realities of the pandemic and political divisions, at least for a few minutes.
Given Dr. Griffin’s statement that he was throwing us a bone, I’ll go for what looks like a good match – Schistosoma – causing schistosomiasis. The symptoms seem like a very good match and the disease is treatable quickly, as in the single day of treatment that Dr. Griffin states for this case, with praziquantel. Of course the 7th Edition of Parasitic Diseases has a thorough discussion of various aspects of the Schistosomes starting on page 379 – highly recommended.
Thanks again for the wonderful content. I look forward to every new show. Stay well.
David
Abingdon, MD
Tim writes:
Daniel, Dickson and Vincent,
The red urine post swim in Lake Malawi is certainly schistosomiasis brought on by an infection of Schistosoma haematobium. The medication is Praziquantel – brand name Biltricide. The life cycle diagrams from your book are helpful thinking about each of these worms.
I spent a couple hours reading up on this after a good read through the PD 7th ed. entry. I’ll spare you the very many odd facts I learned, but I am ready for my first post pandemic cocktail gathering to say the least.
Unfortunately there are no cell assays of S. haematobium to match that of S. mansoni from Wendt/Zhao/Collins et al in the paper discussed today (Science 25 Sep 2020:Vol. 369, Issue 6511, pp. 1644-1649 – A single-cell RNA-seq atlas of Schistosoma mansoni identifies a key regulator of blood feeding) but certainly these technologies will yield a different view of these parasites and biology in general in the coming decade. It is a good time to be a parasitologist as human encroachment is widening niches for these buggers.
I had not realized the scope of the problem until this evening. It might have been an easy case… it was a good lesson.
https://www.cartercenter.org/news/features/h/schistosomiasis/parasite-fighting-medicine-nigeria.html
Best,
Tim
Samantha writes:
Dear Professor Racaniello,
I would like to start off by thanking you for such a wonderfully informative and entertaining podcast series. I am a second year medical student (and a 2018 Barnard grad!) who has been binge watching your videos for the past week since rediscovering your channel. Your podcasts are 1000x more exciting than my online, prerecorded medical school lectures. It’s nice to feel like a Columbia student again after three years, listening to an expert in his field share his knowledge with enthusiasm and purpose. I am very thankful for your and your mission to bring such high-quality educational content to the public.
Regarding Dr. Griffin’s challenge, I believe the teenager has schistosomiasis, caused by Schistosoma haematobium. The main clue that made me think of Schistosoma infection is the patient’s hematuria. Schistosoma is known to infect the bladder, resulting in such bloody urine. Furthermore, this parasitic blood fluke is endemic to sub-Saharan Africa, among other regions, which fits the patient’s recent geographic location. Schistosoma haematobium’s hosts are snails; cercariae from the snails penetrate the skin, migrate to the liver to mature into adults, and then into the vesical venous plexus (which surround the neck of the bladder). The patient’s history of fresh-water swimming is also pertinent positive, since this indicates a potential source of exposure.
We just learned about this parasite in school, so perhaps I have some cognitive bias.
All the best,
Samantha– A very curious medical school student with a newfound love for all things viruses and parasites
Rachel writes:
Good morning TWiP team!
It’s overcast and about 25°F/-4°C here in Indianapolis, and I’m just trying to stay warm. I’m a long time listener but this is my first time writing in, because I’m terrified of getting it wrong. My interest in parasitism is newfound but strong, and I’m so grateful to have a backlog of episodes to go back and make guesses on with instant certification of my answers.
For the young man in Malawi urinating blood, I think it’s safe to say he was infected with schistosomiasis, specifically caused by S. haematobium. This tricky trematode hatches in water and is commonly found in Lake Malawi, especially affecting tourists and expats with less experience with this pathogen. Once infected, the patient will notice blood in the urine as the adult worms infect the bladder.
One day of treatment with Praziquantel will effectively clear up this infection, which I suspect to have been the drug prescribed.
There isn’t a lot of differential for this particular case, as it is pretty cut & dry and can be clinically diagnosed.
Fun fact: this parasite was what initially got me interested in epidemiology and specifically medical anthropology, as it was used as case study in my Introduction to Biological Anthropology course seven years ago. Of course, now come the trials of grad school and my eventual PhD so I can get to the point where I just hang out with worms all day.
Thank you for everything and stay safe!
Rachel
Sources:
https://www.nhs.uk/conditions/schistosomiasis/
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4288699/
Parasitic Diseases 6th Ed (Despommier, Griffin, Gwadz, Hotez, Knirch) pg. 391-418
AK writes:
Good evening esteemed hosts!
A welcome reprieve from all things COVID. I find myself looking forward to TWIP more and more!
I’d say Schistosomiasis Haematobium until proven otherwise.
Incidentally one of my absolute favorite parasites, if such can be said about a disease causing pathogen. It has an absolutely fascinating spectrum of symptoms. We actually find quite a few among our immigrants from refugee camps with diagnosed active or latent tb. Though we find even more strongyloides.
As I recall, we also had a remarkably interesting case a few years back, though quite tragic. A child with neuroschistosomiasis with transverse myelitis, of which the details has slipped my mind.
Stay safe!
A K
ID physician
Byron writes:
Hello TWIP hosts,
It is 32F here in Naperville, Illinois and sunny. Here is my guess for TWIP 191. Schistosomiasis, caused by Schistosoma haematobium. Got to say, it really helps to have the latest PD on hand! Thank you for all the hard work, it has been a lot of fun listening!
Byron
Michael writes:
I’m relatively new to TWIP but I thought I would give a guess to Dr. Daniel Griffin’s case study in TWIP 191 about the teenager swimming in lake Malawi. My guess is at the end of this email.
I started listening in May 2020 to TWIV to learn more about the SARS-COV-2 virus while in lockdown and soon started listening to all the other shows on microbe tv as well. I especially want to thank you for the Virology 2020 videos on youtube which are both informative and also make me wonder at how inventive viruses are through natural selection to adapt and multiply. They are truly amazing and I wish there was a greater emphasis on funding basic science.
Keep up the great work.
Thow
Oakland, CA USA
Urogenital schistosomiasis by parasitic flatworms schistosomes. Also known as bilharzia or snail fever.
Typical treatment by Praziquantel for 1-2 days.
https://www.tripsavvy.com/avoiding-bilharzia-parasite-1454335
https://en.wikipedia.org/wiki/Schistosomiasis
Caroline writes:
Bonjour!
As a first time guesser, I hope this try isn’t too bad, especially since you implied it may be easy.
I’m guessing it is schistosomiasis. A bit of research led me to find that this parasite is endemic in Lake Malawi and so causes many infections in tourists. One common symptom is blood in the urine. The typical treatment for schistosomiasis is usually one dose of praziquantel; sometimes this is split into 2 doses taken within 12h. This treatment matches what was prescribed to the patient in your case.
Thank you so much for all of these podcasts. I have been listening to you for a long time and the episodes keep getting better and better.
Stay safe!
Caroline L.
Water treatment operator
Aida writes:
Dear team at TWiP,
Aida here, writing from Barcelona! I listen excited to each of your programs but this is my first time attempting an answer!
I’m a PhD student in Archaeology at CUNY conducting an archaeoparasitology research, that is, the study of parasitism in ancient populations. Archaeological parasitology is an interdisciplinary field that combines parasitology and archaeological methods to investigate specific patterns of ancient parasite infection in relation to environment, diets, behavior and disease. It also has an objective to trace the origin, evolution and dispersion of the different parasites worldwide and offer epidemiological insights that can help model modern trends. Fascinating field!
My answer to your Case Study for TWiP 191 is bilharzia infection caused by the fluke parasite Schistosoma haematobium. This parasite is widely spread in many countries in Africa including Malawi and it is endemic from the shallow waters of Lake Malawi where there are diverse species of snail that serve as an intermediate host. After asexual maturation occurs within the snail and the parasite reaches the infective larval stage (cercariae), these are liberated in the freshwater. Humans, who are final hosts, can get infected when their skin gets in contact with the cercariae in contaminated waters. These will penetrate the skin finding final “home” in the urinary bladder.
The symptoms range from pain during urination to inflammation of the bladder, including bloody urine as in the case of this week’s patient. The “miraculous” treatment mentioned in the program is a 40-60mg of praziquantel per kg of body weight administered in one or two doses 6 hours apart.
Fun fact, the first ever archaeoparasitological analysis conducted was undertaken by Rufer in 1910 in a 5,000 years old Egyptian mummy that gave positive for S. haematobium!
Ruffer, M. A., 1910 Note On the Presence of Bilharzia haematobia in Egyptian Mummies of the Twentieth Dynasty (1250–1000 B.C.). British Medical Journal 1:16.
Thank you for your fantastic program, I don’t know if I’ll win the book or if my answer is right, but it was fun trying!
Best,
Aida
Alexander writes:
Dear TWiPers,
The young man new to Malawi has probably contracted an infection with Schistosoma haematobium while swimming in lake Malawi. The cercariae swimming in the water during the day penetrate the skin and migrate to the bladder, among other places, where only this species critically causes hematuria. Praziquatel is the drug of choice here.
Interestingly, the characteristic bloody urine was interpreted as a form of male menstruation and a rite of passage for young boys by the ancient Egyptians. Unfortunately, efforts to eradicate this disease in Egypt by mass injection of medications lead to wide spread of Hep C in the country.
All the best to you and all my fellow TWiP listeners,
Alexander, enjoying gentle snowfall at -3°C / 27 F here in Vienna
J writes:
I will start with my guess – schistosomiasis haematobium
Reasoning.
The rest of the family are well but visiting son is not – I assume they had had repeated exposures but the son had not and he showed symptoms.
The 2.5hr drive would take you from Lilongwe, where a visiting aid worker is likely to be based, to the south of the lake. The paper [1] below shows S. haematobium to be endemic to that part of the lake.
This paper [2] points out that S. haematobium targets the urinary tract with hematuria as a common symptom. Link [3] ,to the CDC, shows Praziquantel 20mg/Kg twice a day orally as the treatment which again tracks with the “Given pills, taken morning and night, clears up.”
[1] https://pubmed.ncbi.nlm.nih.gov/8909380/ Schistosomiasis in Lake Malawi
[2] https://academic.oup.com/tropej/article/56/4/247/1650537 Schistosomiasis Haematobium Prevalence and Risk Factors in a School-age Population of Peri-urban Lusaka, Zambia
[3] https://www.cdc.gov/parasites/schistosomiasis/health_professionals/index.html#dx
I have another challenge for you.
In this case I am the patient. I was about 5 years old and travelling by passenger liner from Colombo Ceylon (as it was then) to Southampton UK via the Suez Canal with my parents and younger brother and sister in the early 1960’s. My mother took me to the ships doctor with apparent blood in the urine early in the journey. The MD took blood and urine samples but did not have equipment to run tests but took them ashore in Aden and we picked up results in Cairo. After the visit to the Dr. my parents became much nicer to me and far more forgiving of the problems a very active 5 year old caused them on the ship (including diving into the ships Dr. in the pool and knocking him out). This lasted until we picked up the results in Cairo. This ship was entirely to blame, although my parents seemed to think it was my fault. In the dining room there was a big plate on which there was a Jenga tower made of wafer biscuits, I liked the pink ones, and you could help yourself and the staff rebuilt it ready for me to return for more. Had the Dr. asked me how many pink wafer biscuits I ate a day why my urine was red probably would have been solved earlier.
JJackson
Just a long time TWiV listener dipping into TwiP.
Andrew writes:
Good evening TWIP hosts!
It is a wonderful 12C and clear in Greenville, NC. Which would sound fairly pleasant if my classrooms heater had not broken down here recently leaving the room temperature to be a brisk 18C. Thankfully the county board of education finally transitioned to 100% virtual this week after several harshly written emails about their mishandling of the pandemic.
I have been listening to the microbe.tv podcasts for about 2 or 3 years now and figured I would give this a shot. Please don’t expect anything spectacular from me as I’m a high school science teacher and work part time at the local hospital running the rt-PCR tests for SARS-CoV-2. Granted with the volume of tests being run it certainly does not feel part time.
On to the guess I suppose. After consulting Dr. Google, WHO, and NCBI I am going to postulate the teenage boy has Schistosoma haematobium. I come to this conclusion primarily based on location and the treatment plan. The WHO’s website matched location, and symptoms to the case study.
When looking at treatment I found Praziquantel is the drug of choice meeting that description. For some odd reason I felt the need to make sure the weight of the boy matched a typical teen given the treatment. So again, back to google a typical pill has 600mg, times the 4 pills given leaves us with 2400mg. Seeming how the dosing is 40mg/kg divided into two doses in 12 hours that would make the child in the ballpark of 132lbs or 60kg. This made me feel better about my non medical diagnosis. If it would have been way off I would have kept looking for another alternative.
Just for funzies I did come across a meta-analysis paper on NCBI suggesting that this treatment may not need to be split into two doses over 12 hours and that having the single dose may lead to less vomiting and dizziness as a side effect from the medication.
Thank you for your time and if I happen to win the book I would love for it to be given to my high school here. It would be a fantastic tool to help get students interested in other fields of biology. Many of my students, until we get to our disease unit, don’t even realize humans can get parasites… except for relationships.
Thanks again!
Anthony writes:
Schistosomiasis is endemic in Lake Malawi, perhaps due to overfishing.
Evidence of infection has been found in ancient Egyptiian mummies, The disease was common in Egypt up into the 20th Century. A physician with Napoleon’s army described the blood in the urine as male menstruation.
Did the 1/9 Parasites Without Borders Facebook Post prompt the selection of the case?
Thank you.
Anthony
# # #
“Theodor Maximilian Bilharz, M.D. (1825-1862) was a German physician and an important pioneer in the field of parasitology. Bilharz described the adult stage of Hymenolepis nana and Schistosoma haematobium in human patients that had come to autopsy while he was serving in the German Army medical corps as lieutenant colonel and chief of surgery at Kasr El Aini Hospital in Cairo, Egypt. In collaboration with Karl von Siebold, he made the connection between blood in the urine and infection with S. haematobium.”
https://www.facebook.com/ParasitesWithoutBorders/posts/254337432692631
# # #
Bilharzia in Lake Malaŵi –
What are the facts?
“The open shores (Fig. 1) of Lake Malaŵi were considered free from schistosomiasis
(=bilharzia, bilharziasis, or snail fever) transmission until the mid-1980’s, but transmission is now occurring along shores in the southern part of the lake (Nankumba
Peninsula), and this may be related in part to over-fishing. …
…”
https://ecosystems.psu.edu/research/labs/stauffer/lake-malawi/general/bilharzia$$
# # #
SIR MARC ARMAND RUFFER (1859-1917)
PIONEER OF PALAEOPATHOLOGY
by
A. T. SANDISON
“…
Following these basic observations on normal histological structures Ruffer made
unprecedented and unrivalled observations in the pathological histology of mummy
tissues. Perhaps the most important was his discovery of the calcified eggs of Schistosoma haematobium bilharzia in the straight tubules of the kidneys of two twentieth
dynasty Egyptian mummies (Ruffer, 1910b). This observation is of cardinal importance since it extends back the history of schistosomiasis for three millenia and substantiates the statements in the great medical papyri from ancient Egyptthat haematuria
was common. I suppose this might be regarded as the foundation of a new science of
palaeoparasitology; this science has recently been extended by qualitative and quantitative assessments of helminth ova astonishingly well preserved in medieval cesspits and latrine deposits (Pike, in press).
…”
# # #
The Paleoepidemiology of Schistosomiasis in Ancient Egypt
Helmut Kloos
“…
…. Evidence from the Assyrian boundary markers and the oral history from the time of the Prophet Mohamed suggest that ancient Egyptian physicians and the general population were also familiar with haematuria in schistosomiasis. By the early twentieth century, the Egyptian population was well aware of the widespread occurrence of haematuria to the point where the passing of blood by boys was considered as a normal and even necessary part of growing up, a form of male menstruation linked with male fertility (Girges 1934, 103). T…
…”
http://apjh.humanecologyreview.org/pastissues/her91/91kloosdavid.pdf
# # #
Egypt: The flatworm’s revenge
Louise Sarant
“…
… Haematuria was so common in Egyptian men that French physicians with Napoleon’s campaign in 1798 described Egypt as the only country where men menstruate.
Schistosomiasis is also known as bilharzia after Theodor Bilharz, the German parasitologist who first described S. haematobium in 1851. If untreated, the infection can lead to dysuria (painful urination), haematuria, anaemia and wasting, and is a major risk for bladder cancer, specifically squamous cell carcinoma. This type of bladder cancer is rare worldwide, but it was Egypt’s most common cancer at the start of the twentieth century. …
…”
Sophia writes:
Happy new year!
Thank you Daniel for giving us a case that I can actually answer. I had no clue for the cases presented recently but I was impressed by the number of people who guessed right. They bring the level up: don’t assume that the rest of us are as good!
anyway, my guess is : schistosomiasis. I love diagnoses that can be made with no tests and treatment is easy and available.
You will get loads of answers for this one so I am keeping this short
stay safe and thank you for all you do!
sophia
Leo writes:
Dear Distinguished Professors,
Greetings from the Village of Mendocino on the Northern California coast. Current temperature is 57 Fahrenheit with the fog clearing. www.weather.mcn.org I am just a former winery manager with a lifelong interest in science and discovery. I watched my first TWiV last January and have become a fan of all the Microbe.tv programs.
As to Dr. Griffin’s case presentation in TWiP 191, I think that this adolescent male contracted urinary schistosomiasis caused by Schistosoma haematobium. The blood in the urine is the result of bladder perforations as the parasite releases eggs to be passed through the urine. I have no idea why the rest of the family did not did not become infected. Should they be given a dose of praziquantel “just because”?
It would be fun to use as a differential the African version of a case that allegedly happened in the Amazon. A man was urinating into a river when a small carnivorous fish followed the urine stream and became lodged in his urethra. This reportedly caused pain and a perfusion of blood with or without urination.
I am looking forward to the big reveal.
Wishing everyone health, happiness and long life.
Sincerely,
Leo
Katy-Jane writes:
Dear all,
I’m writing from chilly northcentral Wisconsin, where it is a sunny 6F with a real feel of -3F. (-14C, with a real feel of -19C.) You know, the type of weather where you wonder why you own livestock.
My first thought for the case study in episode 191 was schistosomiasis, but I thought that would be too easy, given that the paper in that episode was also on schistosomes. However, I did not realise that there were many species of schistosome! (I love learning from you all!) The three most common species are Schistosoma mansoni, S. japonicum, and S. haematobium. According to PD7, in the case of S. japonicum and S. mansoni infection, the injury occurs when eggs are deposited in the wall of the intestine and in the liver, whereas infection with S. haematobium, affects the bladder. Bladder infection can result in hematuria, or blood in the urine, which was the main symptom this patient showed, after spending time swimming in Lake Malawi.
According to the CDC website, freshwater becomes contaminated by Schistosoma eggs when infected people urinate or defecate in the water. I know we all know that this happens, but…gross. People are gross. The CDC website also states that vigorous towel drying after an accidental, very brief water exposure may help to prevent the Schistosoma parasite from penetrating the skin. Daniel did make the comment that perhaps the boy had been swimming and maybe hadn’t towelled off quite as vigorously as he should have.
Treatment for schistosomiasis is with a 1-2 day dose of praziquantel.
This all seems to fit, so I am going with schistosomiasis caused by S. haematobium as my guess. Diagnosis could be confirmed by urine sample, although I’m guessing that if the infection is endemic, the medical professionals in the area have probably seen it enough that they don’t necessarily need to confirm the symptoms with a diagnostic assay.
I have made it one of my new year’s resolutions to write in for every TWiP case study this year. I am also training for a half marathon, and I find your podcasts keep me much better distracted from the pain and misery my legs are suffering than music does.
As always, thanks for all you do.
Katy-Jane Shanak
Adjunct Faculty in Veterinary & Dairy Sciences
Northcentral Technical College
Wausau, WI
Martha writes:
Dear TWiP people,
When listening to this episode’s case I was sure I knew the parasite and the treatment. But as is my usual practice I decided to poke about on the internet a bit.
I thought I remembered that the disease had been mentioned in ancient Egyptian papyri and wanted to check that out. For some reason it had lodged in my brain that the disease was so prevalent in Egypt that there was actually a hieroglyph for it and that the ancients equated the hematuria in men to menstruation in women.
Well, turns out the ancient Egyptians did have a word for it; that word apparently is : a-a-a. Ancient doctors seemed to recognize the association with water and advised against standing in polluted water. Not easy with an agricultural system that depends on the yearly flooding of the fields. However the conflation of hematuria and menstruation was made by the French physicians in the Napoleonic era occupation. And I just learned archeologists are finding the agent of this affliction in ancient mummies bladders.
So enough digression, you have a lot of mail to read. I think the young man had schistosomiasis caused by Schistosoma haematobium and was treated with a one day course of Praziquantel.
Thank you all for your work. I thoroughly enjoy your podcast.
all the best.
Martha.
Kevin writes:
When you hear hoofbeats, look for rainbows.
I do detest a chestnut. Likewise for easy phrases, such as ‘slam-dunk’ and ‘no brainer’. Call me a sententious pedant, I can take it.
It wasn’t too long ago that Lake Malawi was considered no-risk for schistosomiasis; just consult the 1992 Lonely Planet tourist guide for Africa. Cetron’s 1996 review, “Schistosomiasis in Lake Malawi,’ also reviews the early 90s consensus opinion that this area was very low risk for transmission. His descriptions of neuroschistosomiasis in two Peace Corps in 1992 quickly changed these perceptions.
The immediate reflex in our current case is to say: Schistosoma haematobium. By the way, this worm should have an identity crisis, having been known variously as Distomum haematobium and Bilharzia haematobium. And let’s not ignore this worm’s erotic potential: two suckers, a gynecophoric canal, and an ‘in copula’ lifestyle. As they say, what could possibly go wrong?
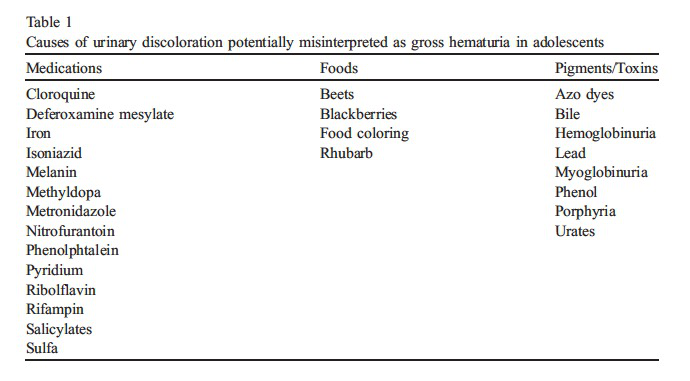
What I find most disturbing in this case is the fact that no diagnostics were run on the patient. Even in the face of the overwhelming likelihood of S. haematobium infection, the importance of objective and definitive demonstration of the diagnosis is never to be devalued. Simply centrifuging the urine and finding ova would be sufficient, though this may be of low sensitivity in light infections. Serologic testing 6-8 weeks post-suspected infection should be attempted. Obtaining hard evidence is crucial in the event that rare complications arise in the future, such as neuroschistosomiasis. Additionally, and as we have repeatedly stressed in previous TWiP cases, the construction of a differential diagnosis is important to avoid premature closure and to account for the possibility of simultaneous or co-occurring pathologies. Non-infectious causes of hematuria in adolescents are listed in the endnotes. Other unusual and unlikely parasitic causes of hematuria are ascariasis, trichinella, myiasis, renal echinococcus; references in endnotes. In our case the patient was doubtlessly given praziquantel, though the CDC states that repeat treatment may be needed 2-4 weeks after initial treatment in order to ensure effectiveness. Additionally, if pre-treatment urine exam showed ova, a repeat urine exam should be performed 1-2 months post treatment.
Which leads me to those rainbows. Colored urine seemed rather fanciful (even if red), especially in view of popular dolls such as Poopsie Slime Surprise Unicorn-Rainbow Bright Star. Something about this TWiP case and a desire for urinary equity with technicolor feces led me to search the string “technicolor urine.” Why was I surprised to find a 1974 JAMA article containing that phrase. I took a chance on rainbow urine. Well the exact phrase wasn’t found, but “‘uroscopic rainbow” was. Now digression has been carried to the level of vice. But there may be a pot of gold at the end of this uroscopic rainbow: see a Terminal Curiosity. And towel off vigorously, even though there’s naught but anecdote to suggest that this works. Exfoliating is invigorating.
Thanks for all that work you do.
ENDNOTES:
Di Bella S, et al. History of schistosomiasis (bilharziasis) in humans: from Egyptian medical papyri to molecular biology on mummies. Pathog Glob Health. 2018;112(5):268-273.
RE: toweling off: CDC
Quickly dry off completely with a towel after an accidental, brief water exposure. This may help prevent parasites from penetrating the skin. However, do not rely on towel drying alone to prevent schistosomiasis. https://wwwnc.cdc.gov/travel/diseases/schistosomiasis
Attention: NEJM 12/19/2019 Perspective article by Hotez et al on female genital schistosomiasis
Ross AG, et al Neuroschistosomiasis. J Neurol. 2012 Jan;259(1):22-32.
Neuroschistosomiasis (usually spinal cord involvement- myelopathy and myeloradiculopathy…. egg laying by aberrant migration of adult worms
Cetron MS,et al. Schistosomiasis in Lake Malawi. Lancet. 1996 Nov 9;348(9037):1274-8.
Purpurowicz Z,et al, Hematuria from urinary ascariasis. Kidney Int. 2017 Jun;91(6):1521.
Quick G, et al Urinary ascariasis in a man with hematuria. South Med J. 2001 Apr;94(4):454-5.
Brunet J, et al , An unusual case of hematuria in a French family returning from Corsica. Int J Infect Dis. 2015 Feb;31:59-60.
Neghina R,et al Reviews on trichinellosis (I): renal involvement. Foodborne Pathog Dis. 2011 Feb;8(2):179-88.
large literature review, case review where 30% of identified cases had hematuria
Ramteke VV, et al. Primary Renal Echinococcosis. Indian J Nephrol. 2017 Jul-Aug;27(4):316-318.
Faridnia R, et al Human urogenital myiasis: A systematic review of reported cases from 1975 to 2017. Eur J Obstet Gynecol Reprod Biol. 2019 Apr;235:57-61. 42 year literature review: 59 urogenital myiasis cases in the world literature.
Gordon C, Stapleton FB. Hematuria in adolescents. Adolesc Med Clin. 2005 Feb;16(1):229-39.
Note on nomenclature:
Theodor Bilharz († 1862 37 years old) – died from typhoid fever in Africa Also, in 1851, during an autopsy, he discovered the trematode worm that is the cause of urinary schistosomiasis, initially naming it Distomum haematobium. 1856 Heinrich Meckel von Hemsbach proposed that the organism be renamed Bilharzia haematobium. In 1858 Weinland proposed the name Schistosoma (Greek: ‘split body’) after the male worms’ morphology, and the name Schistosoma haematobium was officially adopted by the International Commission on Zoological Nomenclature.
Bilharzia: A History of Imperial Tropical Medicine, John Farley · Cambridge University Press, 2003
Non-parasitic causes of hematuria in adolescents:
familial hematuria
exercise induced hematuria
nephrolithiasis
infection
glomerulonephritis
vascular malformation
anatomic malformation
malignancy
IgA nephropathy
hemolytic uremic syndrome
A TERMINAL CURIOSITY
TWiP 191 put me in the mind of pretty colors, and the strangeness of body fluids that are the ‘wrong’ color. It harkens back to simpler times when the diagnostic apparatus was a flask and a physician eyeball, hopefully accompanied by some experience and common sense. Meditating on urinary colors transported me back to the early 1990s when I would see the urinal rims in the Cook County Hospital public toilets that were often bespeckled orange by wayward urine drops from medication adherent TB patients.
As hinted above, urine can take hues from almost anywhere in the rainbow. A modern urine color chart is reproduced below:

Figure 1 Colour chart of urine discolouration. (Foot & Fraser 2006)
14th century uroscopy (Bodelian Library)

urine wheel illustration from 1506
As you can see from the above illustrations, urine was big business in the middle ages. The uroscopy jug was called a matula in Latin (chamber pot, urinal). There are many examples of the urine wheel, a primitive diagnostic aid. The example above is in the Munich Universitätsbibliothek.
Below listed are some references on the spectrum of urine colors that have been reported in the literature. I am leaving out a discussion of a type of colorless ingredient in urine, to wit pneumaturia, where gas is passed in the urine.
A modern urine wheel:
Yellow: Normal urine color is due to urochrome (aka urobilin), a heme degredation product. (Note that urobilinogen is colorless)
dark brown: bilirubin
white: lipiduria, chyluria, pyruia, amorphous phosphate excretion
pink/red: blood, beets, blackberries, rhubarb (in alkaline urine)
smokey/tea colored: hemoglobin (hemolysis) , myoglobin (rhabdomyolysis)
orange: rifampin, pyridium,
blue/green: medications (indomethacin, amitryptiline etc), methylene blue, pseudomonal UTI
purple: chemical reactions in catheter bags related to indigo crystal deposition on the plastic tubing and bags. Intestinal bacterial overgrowth syndrome, Hartnup disease
grey/black: alkaptonuria (oxidation of homogentisic acid). Melanogen excretion and subsequent polymerization due to widespread melanoma and rarely Addison’s disease. Blackwater fever (hemolytic crisis in malaria)
Berman LB. Urine in technicolor. JAMA. 1974 May 6;228(6):753. The familiar color of urine may dramatically depart from yellow to assume various shades of white, orange, green, red, brown, and black. This urinary rainbow contains a treasure of clinical clues to the physician, who reads them correctly. For example, milky white urine may be the result of pus, phosphate crystals, or occasionally chyle. The first two can be separated by centrifugation and then identified microscopically. It may not even be necessary to do this if the urine pH is below 7.0, for phosphates will not precipitate in acid urine. Chyle is also associated with an alkaline urine, and is identified by its extractability with fat solvents. Green urine represents a mixture of blue and yellow. Therefore, a Pseudomonas infection (blue pus) or ingestion of a methylene blue dye will combine with the normal yellow urochrome and emerge as green. The spectrum of red, brown, and black should be separated
Aycock RD, Kass DA. Abnormal urine color. South Med J. 2012 Jan;105(1):43-7.
Chong VH. Purple urine bag syndrome: it is the urine bag and not the urine that is discolored purple. South Med J. 2012 Aug;105(8):446; author reply 446.
Sabanis N, Paschou E, Papanikolaou P, Zagkotsis G. Purple Urine Bag Syndrome: More Than Eyes Can See. Curr Urol. 2019 Nov;13(3):125-132.
Greenberg M. Verdoglobinuria. Clin Toxicol (Phila). 2008 Jun;46(5):485-6. We present a case of green urine caused by ingestion of the cyclic antidepressant amitryptilline and a brief review of the causes for green urine or verdoglobinuria. The possible etiologies for green urine are diverse, however, pharmaceuticals are the most common etiologic agents. While the frequency of occurrence of green urine remains unknown, an awareness of the potential etiologies is essential for the clinical toxicologist to develop a useful differential diagnosis for the problem.
Sauder HM, Rawla P. Beeturia. [Updated 2020 Jun 2]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan-. Available from:https://www.ncbi.nlm.nih.gov/books/NBK537012/ first citation calling for the term ‘beeturia’ is from 1963, BMJ 10-14% of the beet eating population may experience this….due to the excretion of betacyaninins…”it appears to be benign.” NOTE that according to BMJ 10/19/1963 the red pigment is due to betanin NOT acanthocyanin
Beeturia. Br Med J. 1963 Oct 19;2(5363):948-9. This phenomenon (red urine from eating beets) was formerly called acanthocyanuria
Foot CL, Fraser JF. Uroscopic rainbow: modern matula medicine. Postgrad Med J. 2006 Feb;82(964):126-9.
Source of urine wheel illustration: Epyphanie medicorum 1506, Munich Universitätsbibliothek https://viewer.deutsche-digitale-bibliothek.de/index.php?id=1&tx_dlf%5Bpage%5D=4&tx_dlf%5Bdouble%5D=0&tx_dlf%5Bid%5D=https%3A%2F%2Fapi.deutsche-digitale-bibliothek.de%2Fitems%2FGMJDGD2KLAD5SPEDZRHIV25QTTPDH7LI%2Fsource%2Frecord&tx_dlf%5Bpagegrid%5D=0&cHash=5f768ecf578bbb73efd7653eeceb65ea
James writes:
Writing from La Jolla CA, where the sea breeze is blowing, a gentle 50F, 10C. (Back in Denver, it’s snowing. Those poor people.)
My guess with red urine and Africa is Schistosoma hematobium, common in Lake Malawi. In the pathology review course, they gave us the mnemonic that the S. hematobium egg looks a bit like a urinary bladder in shape. Associated with bladder cancer worldwide.
I remembered an “amazon fish” that is reputed to cause hematuria, a candiru catfish that supposedly swims up the urethra and lodges there with its spines. Makes a great legend! Probably not true but still causes a reflex crossing of the legs…http://www.bbc.com/earth/story/20160104-does-the-candiru-fish-really-eat-human-penises
There are other causes of hematuria of course…lots of bacteria, a few fungi, drugs, etc. But this is TWIP!
 | BBC – Earth – Would the candiru fish really eat your genitals?A typical early account describes the candiru as “very small, but uniquely occupied in doing evil”. Such melodrama is common in 19th-century writings on the fish, when a handful of European …www.bbc.com |
| James M. Small, MD, PhD, FCAPAssociate Professor of Pathology and MicrobiologyClinical Career AdviserRocky Vista University |
Chad writes:
For the case in TWIP #191:
I believe that the red urine was a symptom of Urinary Schistosomiasis caused by the Schistosoma haematobium parasite. According to District Laboratory Practice in Tropical Countries by Cheesebrough the haematuria is a common finding of the S. haematobium and is from the eggs, and not the flukes, penetrating through the walls of the bladder.
These parasites are hosted by snails living in Lake Malawi of the genus Bulinus.
Additionally, the fact that the symptoms cleared up after two doses sounds like praziquantel (Biltricide, Distocide). In Principles of Medicine in Africa, the editors mention that it is used and effective with any schistosome species with one or two doses.
My apologies if this guess is way out there. I was trying to investigate using my wife’s text books on the shelves. Usually, I play her the podcast and she just gives me the answer. However, this time she is responding to the humanitarian crisis in Ethiopia, so it was just me and the textbooks.
And if I do happen win the book, are there any “no-picture” options? The hardest part of researching this case was going through the pages of these text books. Medicine is clearly not for me. Although, thank you to all of you who do it!
Bravo Zulu with all the podcasts. Job well done.
Best regards,
Chad
Linz, Austria
Andrew writes:
Kia ora from Pongaroa,
Thanks for the shout out in TwiV-livestream Vincent. You and Amy rock as do all the TwiX podcasters.
The weather is on a roller-coaster – from 29°C two days ago – to 16°C today – to 25°C forecast for tomorrow .
Book: not won yet but I can wait. The signing is going to be a marathon effort and I look forward to it as it will signify the pandemic is almost over.
My case guess: The young man visiting family and swimming in Lake Malawi is schistosomiasis caused by S. Haematobium. Lake Malawi, despite being almost free of the disease up to the 1980s, has endemic bilharzia now. PD7 and the Youtube Parasitic Diseases Lectures #41 tells me that a S. Haematobium caused infection involves the urinary tract which can cause haematuria. Praziquantel is fast acting (one to two days) and treats all schistosome species so I think that is what was prescribed. I have to assume the young man was on vacation from high school or college as it takes some time for the disease to progress to the stage where there would be discoloured urine. A short visit would have not have left time for the disease to progress that far.
There is a possible way that the infection could have occurred quickly and that is to do with a report in IFLScience of the parasite (presumably gravid) crawled up the urethra of a British tourist (I shiver to think about it). This article was originally sourced from a UK tabloid newspaper, so it has to be take with a grain of salt.
Ngā mihi (naa me-he)
Andrew
Allan writes:
Esteemed TWIPsters
Aloha from Kona Hawaii
where it’s currently 80ºF/27C but Mauna Kea, our volcano behind us is covered in snow.
I continue to so appreciate your time and investment in these wonderful podcasts.
Still hoping for a copy of Parasitic Diseases (PD7) so here’s my guess.
I can recall from much work in West Africa 15-25 years ago, that for a teenage boy to have hematuria or frank blood in his urine was often just seen as a sign of sexual maturity or simply coming of age, as it was that common.
A water contact disease, Schistasomiasis (or Bilhartzia if you’re British) is acquired when free swimming cercare from water snails penetrate hair follicles of human skin while one is swimming or bathing in infected water. These cercare migrate to the liver and mature into male and female adult schistosomes where (as Dickson has so wonderful put it), they find each other “delightful” for typically a long and productive life in the venules alongside the intestines or in the case of Africa in the venous plexus of the bladder.
The pressure of 100s of thousands of eggs, often each with a sharp barb, allow them to penetrate into the intestine or bladder but also give rise to bleeding as well… thus the hematuria.
But as we found in several studies in Cameroon, it was only the wealthier boys who would show up with hematuria with those from more impoverished families rarely showing this sign. Why? The poorer boys had to work and never had time to go swim in the nearby ponds on hot afternoons where some peed in the water, shedding Schistosom eggs which were eaten and infected water snails which released the infective cercare…. so they didn’t get infected.
Most often Schistasomiasis is a stealth disease with few if any symptoms, ocaisynly low-grade fever or mild nausea and prior to the early 1990’s the treatments were very toxic. It was Barney Cline, my parasitology professor at the Tulane School of Public Health & Tropical Medicine, that first showed that praziquantel could safely and effectively eliminate Schistosomes from people.
Praziquantel remains relatively expensive and some newer large studies have appeared to show that a home-based 7-day therapy of Artemisinin tea could be as effective with even fewer symptoms and could be much more affordable and sustainable; as this is a disease that still affects 200,000 people per year.
I’m always interested your own stories and of any innovations in the control of Schistosomiasis. I understand the large-scale tests of moluscacides in Egypt to controls the snails never showed that to be a sustainable approach. Any new approaches you are aware of?
Best regards,
Allan Robbins
University of the Nations
Kona Hawaii
Effect of Artemisia annua and Artemisia afra tea infusions on schistosomiasis in a large clinical trial
https://www.sciencedirect.com/science/article/pii/S0944711318305336
Elise writes:
Dear TWiP Trifecta
I’m writing to you from a lower Manhattan in the middle of the first big snowstorm of the year (with “Thundersnow” promised later). It is not horribly cold, however, 28 degrees F (-2.2 degrees C). I will say that while ordinarily, a blizzard is amusing, in the climate of the pandemic, it is reinforcing the feeling of claustrophobia that is too, too familiar these days.
So I believe I have a diagnosis for Dr. Griffin’s case of the teenager with red urine. Ordinarily, I search a little more extensively in case there’s a more elusive solution but I think in this case the most obvious answer is accurate. (Are those famous last words? I hope not.) I think the patient managed to come down with urinary schistosomiasis (AKA Snail Fever or bilharzia) from swimming in Lake Malawi. Schistosoma haematobium is endemic in Lake Malawi where there are many human hosts using the waters that have allowed the parasite to flourish.
My diagnosis is also consistent with the treatment Dr. Griffin mentioned, which is a short course of Praziquantel.
Given that one family member was infected, but the whole family had been swimming in Lake Malawi, was the rest of the family tested and, if infected, treated? Since it is possible to be infected without symptoms, should one be tested, as a precaution?
In terms of prevention future infections, I know that Dr. Griffin recommends “vigorous” toweling off after exposure to potentially contaminated water (though the CDC advised not to rely on this method for preventing infection). I also was interested to read that if it were possible to drink water without it coming into contact with one’s mouth or lips, one would not contract schistosomiasis by swallowing the water. Having said that, clearly this isn’t a stunt to be played around with and one should only drink boiled or filtered water (apparently iodine treatment is insufficient on its own to deal with schistose haematobium).
Did the family continue swimming in Lake Malawi or was this experience enough to discourage freshwater swimming?
As always, many many many thanks for everything you do.
Best wishes
Elise in Lower Manhattan
Anthony writes:
It appears somebody did not take the Doctor’s advice of vigorously drying off after having fun in Lake Malawi!
Final diagnosis: Schistosoma sp.
Anthony
Self taught biochem nerd and pharmacy tech hopeful
Sean writes:
Gentleman,
LOVED Dickson’s story and the devil really is in the details… size matters!- Thank you Dickson. These episodes are fantastic and I cannot say enough about the content you are producing, and the volume!- Fantastic. So much to talk about. Dr. Griffin, thank you sincerely for your tireless updates… they continue to guide us well. Professor Racaniello, your contribution to the biological sciences is without doubt- hoping you get an honorary PhD in the social sciences for all the work you have done across the microbe.tv ecosystem. Your work has kept me informed and focused for over a year know, helping me punch well above my weight in virology and immunology. THANK YOU!
I love Africa and the ‘zebras’ that come with it! Lake Malawi is well known for schistosomiasis, a parasitic blood fluke, which causes many signs including gross painless hematuria.
Fingers crossed.
Thank you,
Sean
Caton writes:
2/4/21
Greetings from the Upper Peninsula of Michigan fellow Tippers,
I would like to express with my appreciation for the engaging participatory learning format of the TWIP podcast. Even though I am not a doctor (I am just a country farmer) I have a strong interest in learning about parasites for many reasons. I have experienced long-term suffering parasitic infection along with many years of undiagnosed Lyme Disease and coinfections. I have found that there is a general ignorance about parasitism and Lyme disease within the American medical community which prevents doctors from even recognizing symptoms of infection. Thank you for sharing your expertise and helping others to learn to recognize and treat these fascinating body invaders.
While excited to hear everyone’s mystery parasite guess letters and awaiting to find out the correct answer in the January 2021 episode, I have to admit that the paper on the RNA sequencing of Schistosoma mansoni made my eyes glaze over. So, I decided to fast forward to get the scoop on the new mystery parasite.
As I listened to Daniel’s “easy” case where a teenager’s urine turns red after swimming in Lake Malawi, I thought to myself, “Hmmm, how will I ever figure this one out?” So, I did the following google search:
“Lake Malawi, urinary blood, parasite”.
My eyes popped when I saw the words Urinary Schistosomiasis. Touché, Daniel– I immediately went back to listen to the paper on the RNA sequencing of Schistosoma mansoni.
My mystery parasite guess: Schistosoma haematobium. According to the NIH, Praziquantel effectively treats all forms of schistosomiasis with 2-3 doses in just one day.
Thank you, Daniel, for your work with Parasites Without Boarders; the support campaign for the Peace Corps Public Health programs; and your endless efforts as a physician and educator at the frontline of this overwhelming epidemic. I am always inspired by your positive spirit and continuous desire to help others.
Caton Gauthier-Nelson
S&C Nelson Farm, Grass-fed Beef
Rebecca writes:
Dear TWIP professors,
Hello from the Parasitology Club at the University of Central Lancashire located in the North West of England, where the weather is cloudy. Many of us at the University are currently busy working through this pandemic, performing COVID19 testing and as part of the population vaccination campaign.
This month we found that there could only be one real suspect for this case. We believe that the culprit is Schistosoma haematobium. Schistosoma haematobium is endemic to Africa, the middle east and Corsica. The young boy has been known to go swimming in Lake Malawi, which has shorelines along western Mozambique, eastern Malawi and Southern Tanzania in Africa. This fits the geographical location of Schistosoma haematobium. Schistosomiasis is the disease caused by the schistosomes such as Schistosoma haematobium and can also be known as snail fever or bilharzia. About 20% of the population of Malawi live in bilharzia-affected areas.
The boy was administered a medication, which was administered 3 times a day. This fits in with Praziquantel which is used to treat Schistosomiasis (Colley et al., 2014) Praziquantel targets the schistosomes calcium ion channels, causing a rapid influx of calcium ions, which results in muscle spasms and complete paralysis in the worm. This, however, only works on the larvae and adult worms.
The other family members were also swimming in Lake Malawi, but they did not become infected with the parasite. This is possibly since children tend to spend more time swimming and may have more exposure to cerceria (King, 2001).
Yours Sincerely,
Rebecca
On behalf of the University of Central Lancashire Parasitology Club
Colley DG, Bustinduy AL, Secor WE, King CH. Human schistosomiasis. Lancet. 2014 Jun 28;383(9936):2253-64.
King, Charles. (2001). Epidemiology of Schistosomiasis: Determinants of Transmission of Infection, p115-132. Imperial College Press, London.
Josie writes:
Dear Triple Trouble Twippers,
After two not-to-terrible but still too wrong answers, I think I have this one. The young man with red in his urine has been swimming with schistosomes in Lake Malawi, and they have found him to be a cozy home away from home. No word on how they feel about a dose of Praziquantal as an eviction notice, as they subsequently left quickly in the dark of night. I like this case because I enjoy folk lore as much as I enjoy science, and so crossover is especially interesting to me. Once or twice over the years Dr. Despommier has mentioned that the ancient Egyptian men who experienced this infection explained it as a male counterpart to menstruation. (Seems no one asked the ancient Egyptian women what they thought when they had the chance.) My two favorite things to learn about, all at once. I love it!
Incidentally, the episodes on schistosomes have also explained something I had always wondered: why I only developed red spots during my second year of Girl Scout camp. At the time I was told it was from swimming in the lake, but no one had an answer for why it hadn’t happened the first year, or the following year, swimming in the same lake. Thanks for scratching that persistent itch.
I was very excited last episode to hear that I have won a book. Altbough I am the only regular listener in the house, at least once a week I get asked if I’ve sent you my address yet. I don’t think I’ll be the only reader when it arrives! I would very much like to have all of you sign it, including Dr. Racaniello, without whom there would be no podcast and therefore no delightfully squidgy science to feed my fascination with creepy crawlies of all shapes and sizes.
My address is included below, and you will find that you can indeed send mail to Library Hell, where books are especially welcome, it being Library Hell. If you look at a map, you will find that Library Hell is located a few hours north of Rich Condit. I call it that for a number of reasons, but mostly because there is no large library consortium such as you enjoy in the northeast. And yes, I’m also one of those pandemic newcomer groupies over on TWIV, brim full of gratitude for science explained by scientists. Maybe I’ll stay after the pandemic, maybe I’ll try microbes or evolution, but TWIP will always remain my favorite. Creepy, crawly, and fantastic.
Thank you for science and some new reading material to boot!
Josie in Library Hell, where the weather is restfully cloudy, 46 degrees Fahrenheit, 7.7 degrees Celsius, 505 degrees Rankine.
P.S. I could have bought a book any time, but I wanted to earn one. I’m sending a small donation in thanks to Parasites Without Borders, in hopes that the book giveaway program can continue and benefit someone who genuinely needs one, unlike me. I’m just an avid reader who likes knowing stuff.
Melissa writes:
Dear Daniel, Dickson, Vincent (and whomever may be joining),
Hopefully I got this in in time for the Feburary episode.
Schistosomiasis (I mean red urine, parasite, sub-saharran lake, what else could it possibly be!), likely S. haematobium, rather than S. mansoni, as the latter tends to present with diarrhea, constipation, and bloody stool.
Treatment is with praziquantel, 40mg/kg twice a day for one day according to the CDC.
(slightly surprised that the child is only ~30kg, given that most praziquantel pills are 600mg and he was given two pills per dose).
I hope everyone is staying safe and sane during the pandemic!
From a windy Toronto,
Melissa (who is very eagerly waiting her turn for the covid-19 vaccine)
Lauren writes:
Hello, TWIP trio
Case study for TWiP 191 of the teenage son of USAID worker with hematuria.
This case study is just in time for Valentine’s Day? Is the liver the Organ of love? At least for the trematode schistosoma. The life cycle of schistosoma; After spending their early life in there lakeside mobile home, (the miracidium peneterates snail) the ceraria leaves, then enjoying a lovely float near the surface of the water of the Lake when our teenage boy gets out of the lake and the water starts to evaporate the cerari slip and slide and enters the skin through a hair follicle. As they go “sightseeing” then migrates in the lungs, settling down to find love in the liver via the bloodstream. For Schistosoma the liver is the place of passion where male and female engage in copula for life, while the male embraces the female. In a sad excuse for a differential our patient could have a UTI or Kidney stone. But, I think he has been playing host to Schistosoma haematobium for awhile enough to develop hematuria. It seems likely with the region and risk of exposure, his chief complaint was red urine not pain. And The clinician just gave him a few pills then it cleared up. The pills might have been Praziquantel. For the rest of the family may not have vigorously toweled off either, so they might need to get a check up too.
Ps. Sorry for anthropomorphizing Vincent but I couldn’t help myself after last twips bookworm response.
Thank you guys for all you do.
Sincerely
Lauren
Owain writes:
Dear TWIP,
Daniel is going easy on us this month! Haematuria after swimming in Lake Malawi makes me think of urinary schistosomiasis, most likely due to Schistosoma haematobium. As well as the praziquantel I presume they were given, I hope they also got a copy of your book to read, so they don’t make the same mistake twice!
All the best,
Owain
Erika writes:
Hi TWiP,
You guys seem to be getting quite popular, so I’ll try to keep this short.
I’m guessing the diplomat’s son was suffering from schistosomiasis and was treated with praziquantel/oxamniquine.
As a crossover reference, I recently convinced my boyfriend to start watching your virology lectures with me. As a musician, he noticed the guitar in the background of your intro. He’s wondering if you play/are any good, or if you want to make some music with him?
Best,
Erika
-9°C, feeling like -16°C in Toronto