
Paul writes:
Diagnosis: zoonotic infection with Dirofilaria immitis; ocular dirofilariasis
Tim writes:
Christina,Daniel,Dickson and Vincent,
Thanks for a great show. I think I was called out as a winner for the TWiP 189 case study… my address and phone number are below if so. Unfortunately my diagnosis was wrong… if that disqualifies me … well this week I am close to sure.
The 50 year old male, kennel and hunting dog purveyor from rural NC had Intravitreal Dirofilariasis a likely human spillover of the common canine heartworm spread by a mosquito vector.
There are several species of Dirofilaria but Parasitic Disease 7th Edition Despommier et. al details Dirofilaria immitis (Leidy 1856) – on page 291 – from the PDF. Immitis is more likely given the fact the patient raised hunting dogs. Dirofilaria tenuis – heartworm of the racoon is also possible (the dogs have to hunt something.)
This link has a video of the removal of a conjunctival infection which I have now watched several times.
https://parasitesandvectors.biomedcentral.com/articles/10.1186/1756-3305-4-41#Fig1
I’m pretty sure I can’t un-watch that… thanks. As things go… I may never leave my SARS2 bunker.
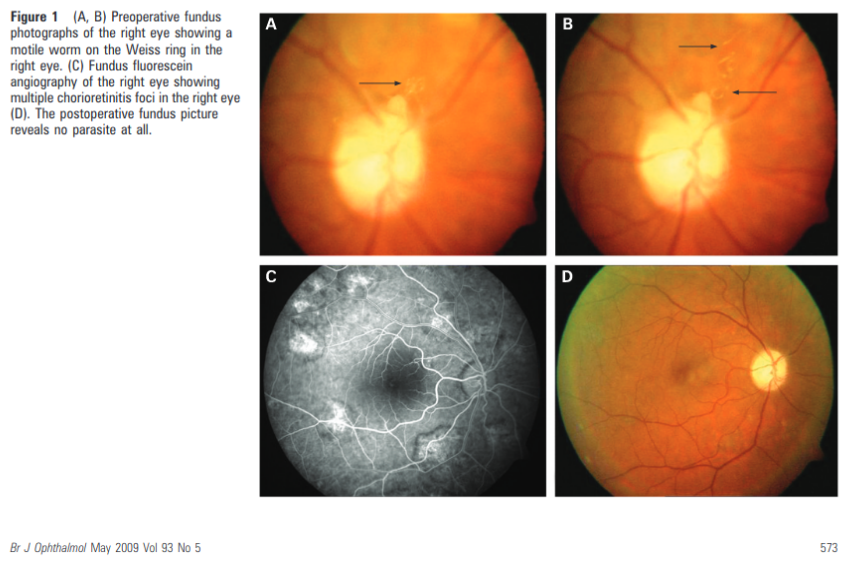
Here are some images taken from the below journal article which is educational in bent – and worth checking out if this guess is right.
This is likely what Dickson saw.
Gungel H, Kara N, Pinarci EY, et al
An uncommon case with intravitreal worm
British Journal of Ophthalmology 2009;93:573-574.
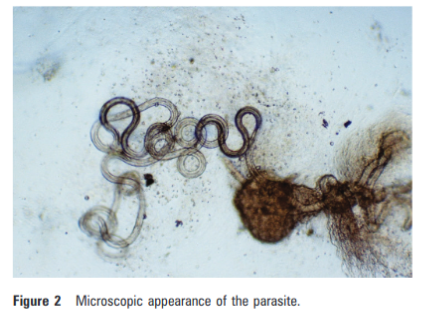
They have a microscopic image as well.
This was curious from that write up.
In humans, the nematode causes a pruriginous subcutaneous nodule, which contains an immature adult nematode. Due to immunological and microenvironmental factors, the parasite cannot reach maturity and is unable to express larvae in the circulation. That is why serology is of little value, and eosinophilia is seldom present.
If this is the case – could you at least speculate as to why this is? That must be why Dickson and his associate were not concerned so much with the parasite?
tJoseph Leidy who named this parasite (I think that is what the parens means in the PD 7th entry) is worthy of his own biography, but I don’t see one. Here is his picture at least. Evidently he was well liked and quite a person. As a 23 year old Leidy became the first person ever to use a microscope to solve a murder mystery. I would have liked to have known him.
I’m privileged to know you.
If indeed I won a book, I’m going to enjoy every minute of it down to the very last footnote. Please let me know the postage/handling fees so I can bonus that back to you in the form of another well earned donation.
Take care,
Tim
Vanessa writes:
Dear TWiP team,
As a first time guesser I am not at all confident on winning the book, however I wanted to email a guess at least once before the show gets too popular to possibly read out all the guesses. Like many of your newly acquired “pandemic podcast partners” I was introduced to your show via the Michael Mina episode and since then I have become an addicted listener of all things TWiV. I have recently completed Vincent’s Virology course on youtube and have now moved onto Brianne’s Immunology course. Unfortunately this order of study means I am still a complete novice when it comes to anything parasitic (a situation I intend to change as a next order of priority).
Anyway here goes my guess – the eyeworm Thelazia californiensis. Of the 30 known species of Thelazia only two species Thelazia callipaeda and Thelazia californiensis are known to cause human infection, with the first being geographically centered on Southeast Asia whilst the latter has been reported to occasionally infect humans in the United States [1]. The clues I used to reach this conclusion were firstly the emphasis from Dixon on how rare it was to see the “entity” and then secondly the fact that the infected gentlemen lived and worked so closely with dogs, the definitive host for these parasites. In fact these infections in humans are extremely rare, with only a handful described in the literature and it is generally agreed that human infection is an accidental event. Diagnosis is usually done via visualization by the clinician and treatment is by the removal of the worms with fine forceps. However in this case it was the early worm that avoided the bird (removal).
Thank you Vincent for all the hard work you put into creating these podcasts. I am a huge fan of Daniel’s clinical updates and I have found it immensely reassuring to see the progress being made in treatment of covid-19 as the pandemic progresses. Dixon, I have to say, you are my absolute favourite. Your cheerful and positive attitude and clear sense of humour is particularly appreciated in these uncertain times.
Stay home, stay safe and keep on educating!
Vanessa (from the UK)
1. Wang, X. L., Guo, J. Y., Wang, X. L., Ma, X. L., Wang, Y., & An, C. L. (2014). Two cases of human thelaziasis as confirmed by mitochondrial cox1 sequencing in China. Pathogens and global health, 108(6), 298–301. https://doi.org/10.1179/2047773214Y.0000000153
Chelsea writes:
Not enough lotion in the world to fix these hands now…
I’m supposed to be doing other work, but could not resist—
Of course after coming up with the answer I immediately went to rewash my already raw hands and am mildly disgusted by my dog (this will pass in an hour).
You describe a man who runs a dog kennel with intermittent non painful blurriness of one eye.
My guess is ocular toxocariasis from Toxocara Canis.
The dog (or cat) have the adult roundworms, and the feces has the eggs. Humans are an accidental host, by inadvertent ingestion of eggs and the larvae can migrate to a variety of tissues. The larvae are unable to undergo any further development and so their lifecycle is terminated wherever they end up- which can cause inflammation or mechanical damage. That explains why no one else has gotten it, I assume they kept better hygiene or did not work with the dogs / infected soil / feces as much.
Although what I’m reading describes a lot of inflammatory reactions, he does not sound like he suffered from anything but annoyance. Maybe that’s because the eye has immune privilege?
I hope it left his optic nerve and perished elsewhere…. Otherwise I would think he did suffer visual loss.
Deworming your dogs and cats is supposed to help kill these pests. Picking up their feces on walks also helps since apparently the eggs can live for years?! And of course, don’t let your kids eat dirt.
Thanks for all the work you do to keep the podcast going,
Chelsea
Leonard writes:
Based upon the association with dogs and dog kennels and the described conditions of the gentleman from rural North Carolina, I am taking a guess that he suffered from toxocariasis. While it is a difficult to confirm the infection since it requires demonstration of larvae via biopsy and we never got that opportunity with the organism moving over the night time hours and since clinicians were unable to conduct any serologic testing (eg, enzyme-linked immunosorbent assay [ELISA], immunoblot) to infer diagnosis because it likely was not known testing during the late 1960’s with regards to parasites, I still cast a vote for this parasite. The organism like came by the gentleman handling soil or sand contaminated with infected animal faeces.
At first blush, I felt this may have been toxoplasmosis but recalled this is associated more commonly in cats than dogs, yet symptoms were the same or very similar to those of toxoplasmosis.
With this being stated, I cast my vote for toxocariasis.
I am a weekly listener to MicrobeTV and the various podcasts that focus attention to virology, parasitology , evolution, and the other interesting scientific conversation held with amazing hosts and guest with every broadcast. Thank you to everyone involved in the ongoing truth and education of the public in such important scientific topics.
Regards,
Leonard
Kevin writes:
Dear Drs. TWiP,
Case guess for TWiP 190: Ocular larva migrans caused by toxicara canis, most likely acquired by fecal-oral consumption of eggs from some of his puppies.
I had a parasite-ridden dream recently in which I led my family through flooded wetlands and–with my dream omniscience–sensed schistosomes honing in on our ankles like heat seeking missiles. I instructed my family to hurry up and, in the fashion of Dr. Daniel Griffin after a dip in Lake Malawi, “towel off vigorously” once we cleared the water. After our trek through the swamp, I was admitted to the hospital for a cancer which for some curious reason they treated with IV-infused mefloquine (an antimalarial).
I know this isn’t This Week in Psychotherapy, but I hope you enjoyed hearing what my brain concocts after reading too much about parasites.
Dreaming of winning the book,
Kevin
Akhar writes:
Good evening from a suitably dark and depressing Stockholm! Hope you all are doing great and are keeping safe.
As we, and I, are still in the deep of it (“it” being the pandemic, the hospitals at capacity and a continuous rise in cases) and I’m on my short daily “alone time”, aka walk home from work, I’ll keep it short.
I usually try to imagine having the case-patient in front of me with no internet or books around and see where my thoughts take me. So this is what I’ve got:
With regards to epidemiology and the signs/symptoms I’d say ocular toxocariasis.
You might find serological positivity for toxocara spp, although maybe not in the 60s(?). And signs of blood eosinophilia might be present. Differentials include loa loa, onchocerciasis, cysticercosis. But not supported by travel history or contact with pigs.
With regards and admiration!
AK
id physician
Michele writes:
Hello!!! The wind is howling like crazy here in LA. It’s a great day to stay in and enjoy the info you all share. You are my favorite edutainment. Thank you for sharing your journal clubs and case studies. My thoughts on #190: Here we evaluate a gentleman who’s risk factors include rural location in North Carolina and contact with many dogs. I’m just a nurse but I’ve heard the saying if there is galloping think of horses not unicorns. My guess is that a roundworm found a home in this mans eye, causing intermittent blurred vision. If I’m wildly off don’t worry I’m listening and learning! All the best and cheers to vaccine roll out! Be safe and well friends, michele.
Wyatt writes:
Hello Twip Drs,
I am sad to say that I missed out on the last case presented, as we were finishing up our Heme/Immuno block this past month at Loma Linda, and I regretfully kept forgetting. I am thrilled to be back at it again. I had a quick question about the Diploma in Tropical Medicine and Hygiene: who is the target audience of this program? Is it primarily for physicians meaning to refine their skills, PhD students looking to research tropical diseases full time, anyone who has taken an interest, or all of the above? It sounds really interesting, and like a lot of fun. It seems that it is to receive certification in the Membership of the Royal Colleges of Physicians of the United Kingdom, but I am not entirely sure how that translates to the health care certification of the United States. If you all know off the top of your head that would be wonderful!
Anyway, onto my guess. I believe that the guilty parasite this month is Toxocara canis, which is a helminth that can be found in North America. Infection starts when the patient consumed the eggs of the parasite, which originally came from the intestinal tract and feces of a dog. The egg hatches in the small intestine of the human, and then punctures the small intestine and migrates out. This now is classified as “larvae migrans”, and is typical of many different parasites. Because this parasite was able to move to the posterior eye, and even lodge itself in the optic nerve, I am assuming that it is one of the visceral larva that can migrate, as opposed to the cutaneous ones. Now the question pertains to where the parasite typically migrates too. Surprisingly, at least to me, these parasites can have typical spots of translocation. Some travel to the meninges, some to the stomach wall, some to muscles, some to the lung and heart, and some to the eyes. Toxocara canis and cati are two that commonly go to the eyes. I arrived at this conclusion because I know that the parasite must be large enough to visualize with a ophthalmoscope, located in the eye, and most likely come from dogs. These qualifiers ruled out Toxocara cati, the cat version of the parasite. There was one other parasite that caught my “eye”, that I had never heard of before: Thelazia callipaeda and californiensis. These cause a primarily cutaneous infection of the eye, and I think that they would have trouble moving to the posterior compartment. I also think that this parasite would be hard to find in North Dakota. T. callipaeda is found mainly in Asia and Europe, and T. Californiensis is found in the western US and is much less common. All this to say that T. canis is my final guess, and hopefully the poor chap is able to be treated. I am guessing they put him on albendazole in order to kill off any of the other worms, however the eye may not respond to the drug regimen. It seems that surgery may have been the best option, but was no longer feasible at the time.
All the best,
Wyatt
Joel and Bronwyn write:
G’day Twiperoos!
Its Joel and Bronwyn here from Brisbane, Australia. Today was a cool and sunny 32°C with the humidity dialled to an oppressive 93%. We’ll try to keep this one short and sweet: it sounds like a case of ocular larva migrans! Our chief suspect for this presentation is Toxocara canis, a dog parasite endemic in the states. According to Otranto & Eberhard’s excellent paper: “Zoonotic helminths affecting the human eye”, the larvae of T. canis are the most common nematode infection of the human eye. They say that children are the most classically affected demographic (as was the case with the 3 year old girl in TWIP 170), but this guys beagle breeding is a bit of an occupational hazard. Dickson told us back waaaay back in TWIP 21 that T. canis stymied efforts to produce germ free beagles.
We were a little confused by the mention of surgical management; UpToDate recommends albendazole, Otranto and Eberhard say photocoagulation therapy can be indicated in cases such as this – where the larvae can be visualised and surgery is reserved for severe cases. But this treatment discrepancy may be a reflection of the vintage of this case, albendazole does not appear to have been in common use in the 60s.
Cheers everyone– we love your work!
-Joel and Bronwyn
Katy-Jane writes:
Dear all,
I’m writing regarding Dickson’s ocular anomaly. The patient raised hunting dogs, so I decided my best bet was to look at zoonotic infections. I found a great article that greatly helped me out (below).
https://parasitesandvectors.biomedcentral.com/articles/10.1186/1756-3305-4-41
I have narrowed it down to Toxocara canis or Dirofilaria immitens. The larval form of T. canis can affect the eye. Known as ocular larva migrans, it is the most common nematode infection of the human eye. The age range is possible for this stage of T. canis infection, and OLM may be caused by few, or even one, infective larva(e). However, it seems that once the larvae are in the eye, they are there to stay, and the damage caused gets progressively worse. (That was just my understanding, I might be wrong!)
Dirofilaria immitens is more commonly known as dog heartworm, for which we (hopefully) give our beloved companions a tasty oral treatment each month. This parasite is prevalent across the US, but particularly in the southeast. According to the article linked above, this species of Dirofilaria has been reported in the anterior chamber of the eye. Furthermore, “Dirofilaria spp. worms are often motile, and noticed by the patient because of interference with vision. Removal is curative and full visual acuity is generally restored with no long term sequelae.” I think this is the one I’m going to choose for my guess.
I found this one a little tricky, and I’m not 100% convinced by my choice of answer, so I’m looking forward to hearing other people’s guesses and the resolution of this case.
Thanks again for all that you do. Wishing you all a wonderful start to 2021 and another year filled with science education.
Oh wait, I forgot to mention the weather! 41 degrees in northern Wisconsin – well above average for this time of year and no complaints here!
Katy-Jane Shanak
Adjunct Faculty in Veterinary & Dairy Sciences
Northcentral Technical College
Wausau, WI
Martha writes:
Dear TWiP, I am a bit late in responding to your latest puzzler regarding the dog breeder in North Carolina in the 1960’s with an eye parasite. I was reminded to write while listening to TWiN. I must admit that most of that podcast goes over my head, but I was struck by a comment by Dr. Calipari, that something can be aversive without being painful. For me, although I am not usually squeamish, looking at eyeballs infected with parasites is aversive, so I delayed responding. I am not familiar with eye parasites. I went looking for images of the eye to acquaint myself with the anatomy. And then on to images of parasite infested eyes, including those opened to better demonstrate the parasite in situ.
I will be brief because my search was rather superficial since I kept closing my eyes ;-). I considered Toxocara canis, which can infest the human eye, but is said to present as a granuloma on the retina. Thelazia callipaeda seems to specialize on infecting the surface of the eye, resulting in some nightmarish images, however not what Dr. Despommier described. So I’m guessing it was Taenia crassiceps which can cause ocular larva migrans in humans and which Wikipedia assures me adult human immune systems typically will remove before permanent damage is done.
Thank you for this and all the TWi podcasts. You may wonder that someone who is too squeamish to look at infested eyeballs would want a book on parasitology. I’m going now to desensitise myself by watching “La Chien Andalou”.
All the best wishes
Martha.
James writes:
through a glass darkly…really think it’s visceral larva migrans from the huntin’ dawgs.
Loa loa came to mind but I don’t recall that going so deep. (that’s one I’ve actually diagnosed on a blood film in an African immigrant who gave the history of a “torpedo” swimming across her visual field.)
There’s lots of protozoa (Acanthamoeba, Toxoplasma, Malaria) that can cause various visual symptoms but I REALLY doubt Dickson could see those in his ‘scope!
| James M. Small, MD, PhD, FCAPAssociate Professor of Pathology and MicrobiologyClinical Career AdviserRocky Vista University |
Dhruti writes:
Dear TWIP team,
My differential diagnosis for the last episode is as per geographical distribution –
Most Likely – 1) Angiostrongyliasis by Angiostrongylus cantonensis
2) Baylisascariasis by Baylisascaris procyonis
3) Trichinosis by Trichinella spiralis
4) Onchocerciasis by Onchocerca volvulus
5) Toxocariasis by Toxocara canis and Toxocara cati
6) Dirofilariasis bt Dirofilaria repens/Dirofilaria Immitis
Least Likely –
1)Loiasis by Loa loa
2)Bancroftian and Brugian filariasis by Wuchereria Bancrofti and Brugia Malayi
Kind regards,
Dhruti
Andrew writes:
Kia ora from Pongaroa,
Covid: New Zealand is buying enough vaccines to vaccinate everyone in the country and more to give to our Pacific Island neighbours. Proud to be a Kiwi.
Weather: An unseasonably cold holiday ~ 15°C and rain
Book: Not won yet. I hope there will be a live stream when you guys can finally get together and sign the books.
Case 138: my guess is ocular lava migrans caused by Toxocara canis.
This is similar to Case 138 which was baylisascaris from raccoons. If the dogs, the man raised, were hunting raccoons this is also a possibility as the eggs might be transmitted by the fur coming in contact with raccoon scat.
Ngā mihi,
Andrew
Erika writes:
Hi,
It’s -5°C and overcast with possible flurries in Toronto.
I started listening to TWiV earlier in the year, for obvious reasons, and TWiP more recently, because parasites are equal parts fascinating and horrifying. I think it’s awesome what you’re doing for science communication, and it’s been great having your extensive archive and regular updates to keep me company throughout our various stages of lockdown. (Also – I grew up in Maplewood, and it’s nice to hear something good coming out of NJ!)
So, with the disclaimer that I have zero relevant training or experience, I’d like to submit my guess for the case study: Baylisascaris infection.
Hoping for a book, and wishing everyone a less bonkers 2021,
Erika
Chelsea on behalf of the University of Central Lancashire Parasitology Club writes:
Happy Holidays TWIP Professors!
It’s another cold and wet day here at the University of Central Lancashire but we’ve been busy trying to solve this case over the Christmas period! We have a number of contenders, though the likely culprit in this case is ocular toxocariasis.
Ocular toxocariasis is mostly caused by the ubiquitous Toxocara canis. As the case states, the patient works with dogs and other animals, which are common hosts for this pathogen. It is likely the patient became infected with Toxocara when they unintentionally ingested faecal eggs or larvae, via poor hygiene practices for example; the larvae then migrated into the eye (Klotz, et al. 2000). Once within the eye, it’s clinical presentations can be classified in one of four forms: posterior pole granuloma, peripheral granuloma, nematode endophthalmitis and atypical presentations (Ahn, et al. 2014). We believe the patient may have suffered from a peripheral granuloma with atypical presentations of optic nerve swelling and other anterior findings: cataract, conjunctivitis.
In some cases, a biopsy of the infected tissue can be used to diagnose OT, however this process is risky and difficult in the eyes. Thus, typical diagnosis involves identifying the clinical presentations of a local granuloma in the retinal posterior pole or periphery. Serological tests can also confirm diagnosis and may include enzyme- linked immunosorbent assay (ELISA) for detection of the serum antibody against Toxocara larvae (Ahn, et al. 2014).
Our second contender for this case is anterior ophthalmomyiasis caused by dipteran flies. Like OT, the larvae can migrate into the eye upon ingestion but is less common in infected patients and clinically appears as anterior uveitis (Sharifipour and Feghhi, 2008).
I was asked to include some eye puns, but the jokes couldn’t be any cornea so I deceyeded against it.
Wishing you all a safe and happy new year,
Chelsea on behalf of the University of Central Lancashire Parasitology Club
Kevin writes:
Dr Despommier, like some film noir gumshoe, had one in the chamber. But the worm got away. Lost to follow-up as the saying goes. There’s nothing funny about this aqueous humor. This whole case is goin’ to the dogs. Last day of the year, therefore a sense of urgency.
Research results in this case are a throwback to the era of anecdote and case reports. Controlled trials are near impossible in these extremely uncommon cases. It’s a refreshing change to read a narrative uncluttered by references to interleukin 23, chemokine receptors and whole genome sequencing. Our 50 year old male dog breeder has not travelled abroad, but I will not let that fact prevent a discursive excursion.
Before a quick differential, I highly recommend the comprehensive Table 1 in Otranto’s 2011 review.
Since our patient hasn’t travelled, the tropical filariases can be ruled out. These usually involve the subconjunctiva and anterior chamber involvement is uncommon. Likewise with gnathostoma, acquired by raw fish eating or copepod ingestion, and usually seen in Asia etc. Many other agents that have been the subject of case reports can probably be eliminated: angiostrongylus, enterobius, dipetalonema, various trematodes, cestodes and cysticerci, pentastomids and maggots (all referenced below):
Leading contenders for Dr Despommier’s elusive worm, in descending order of my estimated likelihood.
1. Dirofilaria. What we know as heartworm. Many species, 2 relevant here: D repens and D tenuis. Larvae are approx 200 microns long. They’ve been described in the anterior segment but are usually subconjunctival.
2. Baylisascaris. Review mentions getting infected via exposure to ‘raccoon latrines’. No, raccoon latrine is not the name of a punk band. Raccoons do not defecate promiscuously, rather they deposit their droppings at designated sites. Our dog breeder may have stepped in it, but infections are uncommon-CDC reported eleven total USA cases in a 16 year period. Note however that the CDC states that dogs can be the definitive host for Baylisascaris and shed eggs, which could have been ingested by our patient. This nematode larva (measures up to 1.8mm in length can cause ocular larval migrans, encephalitis and other serious illnesses.
3.Toxocara. Otranto states that Toxocara spp are probably the most common cause of nematode infection of the eye. Our patient’s intimate connection with hounds makes Toxocara the likliest candidate for his anterior chamber findings. The larva measure 400 x 20 microns. They can be killed by photocoagulation. Serologies are often negative in cases of ocular larval migrans. Treatment usually involves albendazole and corticosteroids.
Final note on treatment. This title sums it up: Eye worm swimming live in anterior chamber: How to remove live nematode without damaging eye structure? Irma Suwandi Sadikin. (simply forceps and lidocaine….)
Various other methods have been reported, some involve ‘paralyzing’ the worm with lignocaine or related drugs, use of simple irrigation/aspiration, and the instillation of viscoelastic substances (e.g. methylcellulose) that gums up the worm for easier extraction. Not a do-it-yourself enterprise.
Happy New Year
ENDNOTES
•General review
Otranto, D., Eberhard, M., 2011. Zoonotic helminths affecting the human eye. Parasites Vectors 2011 4, 41.
extensive open access publication. Starts off with a quote from Seneca. Homines amplius oculis, quam auribus credunt Seneca Ep 6,5 (Men believe their eyes more than their ears) Extensive table outlining specific parasites, transmission/geography, specific eye structures affected and references.
•Nematodes
-GNATHOSTOMA
Nawa Y, et al. Ocular Gnathostomiasis-Update of Earlier Survey. Am J Trop Med Hyg. 2017 Oct;97(4):1232-1234. Collection of 73 cases from international group of authors. Gnathostoma: food borne (e.g. raw fish, raw wild boar, raw lobster consumption). Male:female case rate= 9:1
Diaz JH. Gnathostomiasis: An Emerging Infection of Raw Fish Consumers in Gnathostoma Nematode-Endemic and Nonendemic Countries. J Travel Med. 2015 Sep-Oct;22(5):318-24.
Benavides MA, et al. Case Report: Ocular Gnathostomiasis in Venezuela Most Likely Acquired in Texas. Am J Trop Med Hyg. 2018 Oct;99(4):1028-1032. Worm was in the corneal stroma.
-BAYLISASCARIS
Gavin PJ, et al. Baylisascariasis. Clin Microbiol Rev. 2005 Oct;18(4):703-18. Comprehensive reference with abundant illustrations / photographs…Humans become infected by accidentally ingesting infective B. procyonis eggs from raccoon latrines or articles contaminated with their feces….(! where does one, why does one dabble in raccooon latrines?)…Once invasion of the central nervous system has occurred, the prognosis is grave with or without treatment. To date, despite anthelmintic treatment of cases of B. procyonis neural larva migrans, there are no documented neurologically intact survivors…Ocular disease in Baylisascariasis: Ocular disease in baylisascariasis occurs in association with severe NLM or as an isolated finding. Most infants and children with clinical VLM and NLM also have evidence of ocular disease. Here, visual impairment or blindness results from widespread larval migration, with destruction of the visual cortex, or from larval migration within the eye itself. Ophthalmoscopic exam demonstrates choroidioretinitis, optic neuritis, or atrophy and occasionally may reveal motile larvae migrating within the retina (21, 31, 39). Morphometric measurement of retinal larvae allows differentiation of the larger B. procyonis larvae (1,500 to 2,000 by 60 to 70 μm) from those of related Toxocara spp. (350 to 445 by 20 μm), which are a somewhat more common cause of isolated OLM (21). Baylisascaris is now considered the most common cause of the large nematode variant of diffuse unilateral subacute neuroretinitis (DUSN), a form of OLM associated with progressive monocular visual loss and changes in retinal pigmentation and optic nerve anatomy (21, 39). Severe localized ocular damage results from inflammation of the retina, retinal vasculature, and optic nerve in response to the local presence of B. procyonis larvae (21, 31).
Sircar AD, Abanyie F, Blumberg D, et al. Raccoon Roundworm Infection Associated with Central Nervous System Disease and Ocular Disease — Six States, 2013–2015. MMWR Morb Mortal Wkly Rep 2016;65:930–933 several descriptions of eye involvement, though not specifically anterior chamber involvement.
–FILARIA (VARIOUS)
Diaz JH. Ocular Filariasis in US Residents, Returning Travelers, and Expatriates. J La State Med Soc. 2015 Jul-Aug;167(4):172-6. (full text not available) Clinicians should maintain early suspicion of ocular filariasis in US residents, returning travelers, and expatriates who complain of combinations of red eye, eye pain, foreign body sensation, reduced visual acuity, and migrating ocular worms, even without significant peripheral eosinophilia or microfilaremia …Mobile adult worms trapped in the subconjunctiva or anterior chamber should be removed by ophthalmologists to permit species identification, prevent posterior uveitis and iritis, and stop worm migration into the posterior chamber which could require lens removal and vitrectomy for worm extraction causing further eye damage. pests mentioned: Dirofilaria repens, Dirofilaria spp, W. bancrofti, B. malayi, O. volvolus
Khan N et al. Worm in anterior chamber of the eye. BMJ Case Rep. 2018 Mar 23;2018:bcr2017223173. Open access. Intraocular infestation by live L. loa is a rare occurrence, and few such cases have been reported previously. case of live L. loa in the anterior chamber which was surgically removed under topical anaesthesia…the authors’ differential dx: Wuchereria bancrofti, Brugia malayi, B. timori and Onchocerca volvulus.
Kale P, et al Ocular dirofilariasis: Series of three cases and review of literature. Indian J Med Microbiol. 2016 Apr-Jun;34(2):264-5 This article is a brief correspondence. The worm was subjunctival / periorbital in these cases…
Montesel A, eta al There is a worm in my eye! Ocular dirofilariasis. Eur J Ophthalmol. 2019 Sep;29(5):NP5-NP8. more subjunctival involvement
Pradhan D,et al. An Encounter with a Worm in Anterior Chamber: A Case Report. Nepal J Ophthalmol. 2018 Jan;10(19):98-101.
Authors state that ocular involvement with helminths usually involves the conjunctiva or subretinal space. Anterior chamber involvement is very rare. Case here conjectures that the worm seen was Dirofilaria, though they were unable to definitively identify the organism… worm was 2.5mm long…there are 6 species of Dirofilaria that can infect humans…D. repens is commonly found in subcutaneous tissues of dogs, foxes and cats, while Dirofilaria immitis inhabits right ventricles and pulmonary arteries of dogs and cats hence, also known as dog heartworm. Aedes, Armigeres, Culex, Anopheles, and Mansonia species are intermediate host cum vector for this nematode. Ocular involvement is usually periorbital, orbital, subconjunctival or subtenon (Chopra, 2012). However, there are very few intraocular lesions have been reported
-ANGIOSTRONGYLUS
Tiwari US, et al Angiostrongylus cantonensis in anterior chamber. Indian J Ophthalmol. 2019 Jan;67(1):158-160. Live worm in anterior chamber is a rare finding. We hereby report a case of ocular Angiostrongylus cantonensis, which, to the best of our knowledge, is the third case report from India. A 70-year-old female presented with the complaints of watering and foreign body sensations in right eye since 2 months… a translucent worm of approximately 15 mm length was found freely moving in anterior chamber. Patient underwent surgical removal of live worm, which was identified as A. cantonensis. ~1% of Angiostrongylus cases have ocular involvement…Ocular involvement includes optic neuritis, blepharospasm, uveitis, macular oedema, retinal oedema, necrotic retinitis, panophthalmitis, papilloedema and optic nerve compression…..humans, the incidental host, can acquire the infection by ingestion of L3 larvae via raw fish, molluscs, reptiles and amphibians or via vegetable matter contaminated with L3 larvae…article with an alarming photo of the worm in the anterior chamber…must read the ingenious operative technique that ensnared the worm in a viscoelastic substance…
TECHNIQUE OF PARASITE REMOVAL: Patient underwent surgical removal of live worm under topical anaesthesia. A paracentesis at 9 o’clock meridian was made followed by intracameral injection of lignocaine 2% (0.1 mL) to anaesthetise the worm. Hydropropyl methyl cellulose (HPMC) injected to prevent damage to adjacent structures, to maintain the space and to protect the endothelium. The worm got embedded in the viscoelastic substance, which minimized the risk of damage to iris and cornea. The worm was removed .The viscoelastic washed out of anterior chamber; balanced salt solution was injected to reform anterior chamber.
-ENTEROBIUS
PINWORMS in the eye. Gross
Babady NE, et al Enterobius vermicularis in a 14-year-old girl’s eye. J Clin Microbiol. 2011 Dec;49(12):4369-70. 3 worms in the conjunctival sac…went to the ER….got (!) cipro ophthalmic solution
-DIPETALONEMA
Beaver PC, et al. Dipetalonema from the eye of a man in Oregon, U.S.A. A case report. Am J Trop Med Hyg. 1980 May;29(3):369-72. a 21mm worm was retrieved from the right eye of a 32 y/o man. Worm identified as an L4 larva of a Dipetalonema spp nematode. (In a strange example of nominative determinism, Prof Beaver states that this specimen closely resembles D. sprenti Andersson 1953, which was found in a Canadian beaver.)
•CESTODES
Andreoli MT, Farooq AV, Mieler WF. Asymptomatic Intraocular Mass. JAMA Ophthalmol. 2016 Jan;134(1):105-6 case report of intraocular cysticercosis. wrong area though….posterior chamber.
Aghamohammadi S, et al Intraocular cysticercosis by Taenia crassiceps. Retin Cases Brief Rep. 2008 Winter;2(1):61-4. Case of a 14 y/o girl in Oregon with 30-40 T crassiceps larvae in the posterior pole of the left eye
Yadav RY, Ghosh A, Sharma K, Ahmad S. Atypical presentation of live cysticercus larva in anterior chamber. J Indian Med Assoc. 2013 Apr;111(4):264-5. 25 y/o woman with a right eye mass in the anterior chamber
•TREMATODES
Dalimi A, Jabarvand M. Fasciola hepatica in the human eye. Trans R Soc Trop Med Hyg. 2005 Oct;99(10):798-800. 44 y/o woman in Iran had a fluke identified as F. hepatica in the anterior chamber of her left eye. Very convincing picture also shown...
•MISC
-pentastomid
Lazo RF, et al. Ocular linguatuliasis in Ecuador: case report and morphometric study of the larva of Linguatula serrata. Am J Trop Med Hyg. 1999 Mar;60(3):405-9 34 y/o woman with a mobile mass in the anterior chamber
-ophthalmomyiasis (ocular myiasis)
Georgalas I, et al. Intraocular safari: ophthalmomyiasis interna. Clin Exp Ophthalmol. 2011 Jan;39(1):84-5. 27 y/o woman with a subretinal and an anterior chamber maggot, acquired on a safari in South Africa. Similar to Dr Despommier’s case, the maggot migrated into the posterior chamber and was “shot” with a laser. Culprit believed to be a botfly (Oestridae). Good photographs and reference list. This case report lives up to its adventurous title.
from my TWiP 169 endnotes:
Table from Rathinam 2011 (Intraocular Parasitic Infections, S. R. Rathinam,, Ocular Immunology & Inflammation, 19(5), 327–336, 2011)
| Anatomic location | Clinical manifestation | Infectious organism |
| Orbit Conjunctiva Anterior chamber Iris Vitreous Subretinal space Retina | Orbital Cellulitis Subconjunctival (SC) motile wormSC cystSC granuloma Alive motile wormHypopyonHyphemaAnterior chamber granuloma Iris atrophy, Iris holes Alive wormIntact mobile cystPanuveitis Subretinal motile wormCystMultifocal chorioretinitis with new crops of retinitis RetinochoroiditisRetinochoroidal granuloma | Dirofilaria DirofilariaCysticercosisTrematode granuloma GnathostorniasisRuptured cysticercosisGnathostorniasisTrematode granuloma Gnathostomiasis GnathostorniasisCysticercosisRuptured CC DUSNCysticercosis DUSN Toxoplasma gondiiToxocara |
A TERMINAL CURIOSITY
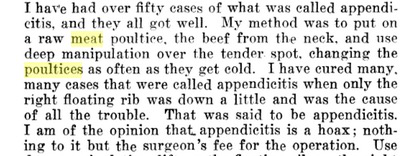
Digressive to the point of pointlessness, but this mental pathway was stimulated by the known (especially by Dr Despommier) phenomenon of frogmeat and snakemeat poultices and the association with ocular sparganosis (mercifully omitted from the above discussion) and tediously expounded upon in TWiP 169’s Terminal Curiosity. The subject of poultices brought to mind the whole gamut of devices (touched upon in TWiP 189 talk of cholera belts and such…) to wit waistcoats, girdles, belts, stomachers, cummerbunds, wraps, compresses, plasters, poultices and fomentations..I suggest reviewing Dr Despommier on frog poultices for the Columbia University online magazine 21st C: http://www.columbia.edu/cu/21stC/issue-2.1/despomm.htm
Want of time and interest in the preservation of mental dignity, this capacious topic is served here by the puny fragments below offered:
Rattlesnake bites may be treated by killing a chicken and wrapping the warm body around the bite to draw the poison out.
https://www.tshaonline.org/handbook/entries/folk-medicine (Texas State Historical Association)
a youtube video advocating the use of a raw meat bandage https://www.youtube.com/watch?v=rsPPkV0X–8 [ I condemn the practice!]
Spinology, The Key to the Secrets of All Science of Healing, W. Riedl, 1911
Flannel fomentation–The Diseases of Children Medical and Surgical, Henry Ashby, George Arthur Wright, London: Longmans, 1905 “Hot fomentations: Flannel or spongio-piline may be used, being wrung out of boiling water in a towel, sprinkled with laudanum or turpentine according to the effect desired, and applied. The fomentations should be retained in position by means of a flannel bandage.”
Goodholme’s Domestic Cyclopaedia of Practical Information, Goodholme, Todd, C Scribner’s Sons:New York 1889 “A thin slice of raw meat bound to the part is said to remove the discoloration quicker than anything else…If the contusion is severe and inflammation threatens, warm bread poultices or hot flannels may be applied…”
Man’s best friend? Diseases of Man Acquired from his Pets, B. Bisseru, Heinemann:London, 1967
Elise writes:
Dear TWiP Trifecta,
I am writing to you on New Year’s Eve from Lower Manhattan, and wishing you all a better 2021 than the year that is finally departing. It is a damp-isn 39 degrees F (3.9 degrees C) here at the bottom of the island.
I am not confident in this diagnosis but after missing the previous opportunity, I’m determined to submit one. It was hard for me to sort out which sort of parasite Dickson saw in the patient’s eye, but given that it was causing intermittent blurred vision in the evenings, I suspect that it was a helminth. Dickson was very gleeful about what a sight it was, so I know it was easily visible, and worms in the body always seem to be more lively at night.
A few parasites do show up in human eyes, and I suspect that the infection might be toxocariasis, given that the patient ran a kennel and had a lot of exposure to a lot of dogs. My diagnostic lack of confidence comes from the fact that I read that ocular toxocariasis can damage the retina, and if this gentleman never got it removed perhaps the outcome was worse than was implied. The recommendation would have been to remove the worm, but this one wandered off and I don’t know if it would cause more problems.
While I did find other discussions of helminths that show up in human eyes, toxocara seemed to be the most likely given the lone symptom, but as I said, I’m not entirely confident.
As always, many best wishes to all of you. Thank you for all of your podcasts and all of your work that keeps me engaged, distracted from less pleasant thoughts and utterly interested.
All the best and happy happy New Year,
Elise (Mac Adam) in Lower Manhattan
P.S. I know this is a crossover reference, but Vincent, I was on the Upper East Side this week and thought of TWiV because of this sight that you mention with some nostalgia.

Josie writes:
Dear Triumphant Twipmaster Trio,
It seems that writing answers to your parasitic puzzles is becoming the way I pass my time while biology takes over my life. Last time I wrote in I was recovering from oral surgery (blame my bad answer on the codeine), and now I’m writing while quarantined, waiting out my time while my essential worker husband gets a fourteen day break from his essential work. Good thing I like medical science, since I am using so much of it lately!
As far as Dr. Despommier’s mystery case goes, it is very clear to me that the man with the blurry vision has become a dead end host for a book worm. Normally devouring any available reading material, this poor creature must have been munching happily away at the evening newspaper the unwitting host also enjoyed devouring, was accidentally consumed, and migrating through various organs ultimately settled in the host’s eye, because there it could see out and continue reading whenever the man himself also sat down to read, this inadvertently causing visual distortion for the host as the view was now somewhat blocked.
Seriously, though, I seem to remember that the man raised hunting dogs, implying contact with raccoons either because they are the intended prey, or because they are helping themselves from the dog’s dinner. Could the mystery worm have been Baylisascaris, contracted by contact with raccoon feces (or whatever surface the feces was deposited in a week or two before)?
Weather here in Library Hell is currently a comfortably chilly 39 degrees Fahrenheit, 4 degrees Celsius, and 3 degrees Reaumur. For the occasional complainers that have grumbled about your weather reports over the years, they should know better. All good scientists take note of their field conditions and record them as part of their work.
Happy vaccinated New Year,
Josie in Library Hell
Leland writes:
Hope this gets in in time.
Ocular larva migrans – Toxocara canis.
Caton writes:
Happy New Year, Twippers. It is a beautiful sunny winter day with a white blanket of snow here in the UP (Upper Peninsula of Michigan). The icicles are melting this mid-morning and the thermometer reads 40 degrees.
Although I am just a country farmer, I still would like to give a guess of the identity of the “entity” that haunted a beagle breeder’s eye in the 1960’s. First, I would like to to point out that as Dickson presented this case study, he said that he saw the mystery “entity” with his own eyes and said he was 95% certain of what it was. Yet, he gave us no description of size, shape, or color of the organism. I believe he omitted that information because revealing it would make this exercise way too easy.
I believe Dickson saw some sort of zoonotic roundworm that had migrated to the gentleman’s eye. I am 95% sure that it was the canine species, Toxocara canis, because about 30% of dogs younger than 6 months deposit Toxocara eggs in their feces.
Other animals have their own species of roundworms that can also find their way to the human eye, such as cats (Toxocara cati) and raccoons (Baylisascaris procyonis). Both could have been possible candidates for the gentleman’s infection in his southern rural environment.
Lastly, if the gentleman had traveled abroad, say, to Africa, he could have gotten Loiasis, also known as the African eye worm. It is caused by the parasitic worm Loa loa and is passed on to humans through the repeated bites of deerflies (also known as mango flies or mangrove flies) of the genus Chrysops. The Loa Loa worm most commonly migrates to the human eye but can also invade other parts of the body. The following video shows the removal of a Loa loa worm in the eye. It is both fascinating and educational.
I have to agree with Dickson–the study of parasites is endlessly amazing.
Caton
S&C Nelson Farm, Grass-fed Beef
Viki writes:
Hello beloved twippers! It is 19 degrees F in Duluth, sunny, but a chance of snow tomorrow!
I received my used copy of the second edition of Parasitic Diseases last week. On the first page of the table of contents someone had written “No more lettuce,” and I hope that advice is no longer relevant. I was relieved to see that the images are black and white, as vivid images could give me nightmares.*
I guessing that this poor fellow has ocular toxocara migrans, not as uncommon as I would wish. People going to see an ophthalmologist for vision problems have this at a rate of between .1 and 1 % in warm climates. The American Journal of Tropical Medicine and Hygiene calls this a neglected disease. Sorely neglected.
I’m pretty sure that I read somewhere that Toxocara larva don’t migrate to the optic nerve, so does this indicate that my guess is wrong or that this migration is new to science? What other larval parasites migrate to the eye? As far as treatment, Albendozole or Mebedozole are recommended but not FDA approved (as of 2014), and steroids for inflammation.
I’m worried about this fellow’s vision and anxiously await your podcast.
*My dear friend Jean, when she was a child 60 years ago near the Canadian border, used her precious few coins to go to the feed store and buy deworming medicine for the barn cats and dog. It sounds as though she would see dead worms in their feces. She thinks that she has developed a parasite phobia, but I don’t see how that’s possible—negative feelings about parasites are normal. She grew up to run the chemistry lab at one of our local hospitals. Coincidence?
Yours in parasitology,
Viki
Alex writes:
Dear Professors,
just after listening to your latest episode in which Prof. Despommiers presented a case of a patient with an ocular parasite, my podcast app presented me with an older episode, namely number 40, which is aptly titled “Doctor, there’s a worm in my eye!”. This of course made the diagnosis a lot easier for me: the patient most probably suffered from a case of ocular larva migrans syndrome from Toxocara cani. As a dog breeder, exposure is quite clear in this case. Differentials include Loiasis, Onchocercosis, Cysticercosis and gnathostomiasis, but all those nasty buggers are very rare in the US. That said I must say that I envy you for having seen this fascinating creature in the flesh. Such an occurrence should be enough to turn anyone into a passionate parasitologist. Take care and all the best,
Alexander, 3°C/38F and cloudy in Vienna
Kate writes:
Hello!
This is a guess for episode 190, the man with the blur in his vision. I believe he had ocular larval migrans caused by Toxocara canis. I’m writing to you from the parking lot of our pediatrician waiting for my daughter’s appointment, but I didn’t want to forget to write in! Maybe I can win “shortest guess.”
Thanks!
Kate from Knoxville, TN (gorgeous day here today!)
Owain writes:
Dear TWIP,
To my shame, I didn’t submit a case guess last month! Apologies for the absence.
My guess for this month’s case is a worm of the genus Toxocara, most likely Toxocara canis given the known dog exposure. I don’t know of many other worms that get into the eye as described, although Taenia, Onchocerca and Loa loa all cause slightly different kinds of eye infections. If you have time, a brief overview of eye worm infections from you experts would be great!
A brief question for Vincent – I am using the dedicated MicrobeWorld app to listen to the podcasts, it works very well! But sadly, I can’t see your newer podcasts like TWIEvo and Immune on there. Is this just because I’m doing something wrong from a technology perspective, or are they not uploaded onto the app? I’m not as good at technology as I am at eye worms..!
Hope you’re all well!
Yours sincerely,
Owain