
Case guesses:
Bruce writes:
Dear TWIP,
At the beginning of the Pandemic I became curious as to what a virus is and by doing a Google search on “Viruses”, ran across Vincent’s virology lectures. It has been a struggle but after numerous months have gotten up to lecture #14 with some comprehension. Luckily, no one is grading me.
I think the virology lectures introduced me to TWIV which I listen to weakly and enjoy Daniel’s up to date information on Covid-19. Out of curiosity, today I just listened to TWiP 189: Toe jamming’ and the case study presented by Christina on the women with the swollen abdomen. I’m a soon-to-be retired Medical Sonographer and the case description reminded me of Cystic Echinocccosis (CE), also known as hydatid disease about which we learned about in school some 35 yrs ago. I have never knowingly seen a Hydatid cyst but, after reading up on it, I think it is somewhat consistent with the patient’s clinical presentation.
1) Cystic Echinoccosis is caused by infection with the larval stage of Echinococcus granulosus, a ~2-7 millimeter long tapeworm found in dogs (definitive host) and sheep (intermediate hosts). Christina stated the patient was exposed to a dogs and sheep.
2) CE is characterized by a slow growing cyst in liver or lung. A slow growing cyst in an obese patient may go unnoticed initially, enabling it to get to 20cm.
3) CE may appear as a swollen abdomen.
4) Pt may be asymptomatic for years, or could experience pain and jaundice.
5) The worm is found in Africa, e.g., Ghana.
6) CE may be misdiagnosed as liver cancer.
Christina stated the lump was firm and did not appear to be fluid filled.
This may not be consistent with a Cyst but maybe palpation in an obese pt could be misleading.
I think the diagnostic test may have been an ultrasound exam.
Thank you Vincent and all others involved for exposing me to viruses, parasites, etc. I really value your efforts.
Bruce
San Jose, California
It finally rained in San Jose today.
Tim writes:
Greetings TWIP,
This paper (cited below) reports liver flukes in Ghana in 2014. I know it is a stretch but … following in Parasitic Disease 7th Edition Despommier et. al (yes Griffin is an al.) pages 405 and following… meh…this seems to fit. A quick google bridged the SE Asian worlds to Ghana with this report. Where there is one … there are many.
If I am right.. then this paper is the a great one to explain… the discussion is quite well done. If I am wrong it’s still a good discussion.
Asare, K.K., Boampong, J.N., Ameyaw, E.O. et al. Microscopic identification of possible Clonorchis/Opisthorchis infection in two Ghanaian women with undiagnosed abdominal discomfort: two case reports. J Med Case Reports 8, 369 (2014). https://doi.org/10.1186/1752-1947-8-369
Christina asked for the field diagnostic. Light Microscopy of fecal specimen fits the bill.
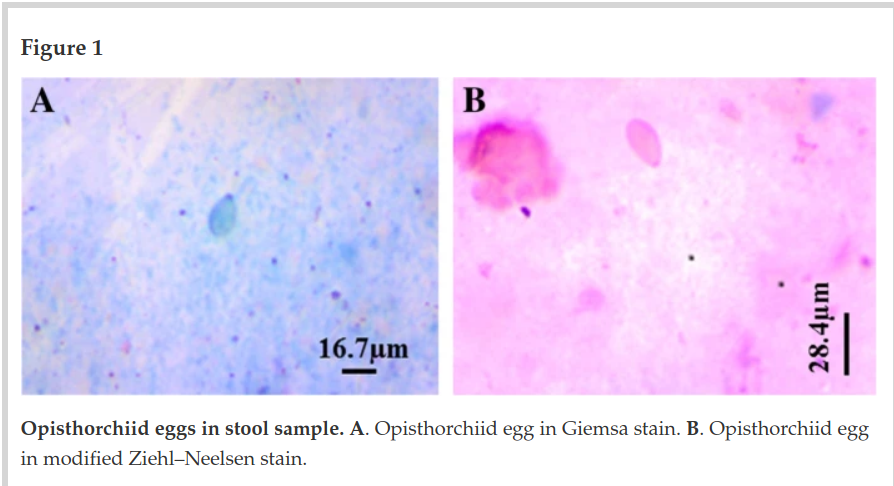
Page 409 (at this rate I won’t need a book if I win one…as I seem to be averaging about 50 pages a month… this one took me about 100 pages to ferret out) gives the final hint. I’m not sure what the 20cm smooth non compacting ball is other than a bunch of worms – Clonorchis sinensis I presume.
Here is my bio for the month… Dr. Francisca Mutapi. These are fun.
I’m hoping I am wrong here. I have much to learn and failure is the best teacher in all things.
Dan/Christina/Dickson/Vincent – best
Carry on,
Tim
K writes:
Hi,
Looking a little deeper into the parasite realm, I found a few too many scary possibilities. Without a firm parasitology background, I dove in free of the shakels of experience and knowledge and into the domain of best guesses based on scary looking pictures from the internet. In my travels, I found what I think is the cause; Subcutaneous Cysticercosis.
The large firm mass on her trunk was the leading piece of evidence. As was the fact that she was from Ghana and lived as a subsistence farmer which could put her into contact with the eggs from Taenia solium, the parasite responsible.
I believe I was the winner from the episode on T. gondii, so I forgo any chance at winning for this round. But I still wanted to have a guess, but for equity sake, please don’t put my name into the draw. But feel free to read my entry on your next podcast.
Active Listener.
Masked in Edmonton.
K
Anthony writes:
I am writing in once again to provide my guess for the case in episode 189
I was initially tied between Echinococcus and Entamoeba – but as the patient appears to have very mild symptoms (extremely atypical for progressed amoebic dysentery – you would normally be screaming in pain at that point!) and is a farmer by trade I’d likely suspect it is either hydatid disease or some sort of weird liver fluke of the genus Fasciola
Both diseases however have the same treatment: A combination of praziquantel and albendazole plus surgical removal of any cystic material left after drug treatment
Hope all is going well (I’m planning on trying to get my Certified Pharmacy Technician diploma soon!)
Anthony
James writes:
Respected professors,
I am a first time writer into twip. I have a guess for the case in episode 189, but I must first make a few positive comments. Thank you Dr. Griffin for getting me a copy of Parasitic Diseases this past summer, you may not recall but we had a few shipping issues and email exchanges before I finally received the book. To make up for the time delay on my order you sent me 2 extra copies, I hope you will be happy to hear that I gave them to a PGY4 and medical student who are pursuing infectious diseases. I am an intern, so time is fleeting and I am only occasionally able to listen on jogs or commutes which don’t allow for promptly writing in. However, recently, I heard Viki writing from Duluth, Dr. Dommer from Ashland, and Courtney from Omaha. I did my medical school and undergrad in Duluth and made several trips to Ashland to kayak on the beautiful Lake Superior, and now am an intern in Omaha. I hope you all realize what an awesome community you have established through these podcasts. When I listen, I feel in touch with my local community and also get to hear from those writing in from all over the world. What a cool opportunity!
Now for the case. My guess is that this lesion mistaken for a hernia is a case of onchocerciasis which is an infection with the nematode Onchocerca volvulus which is known to be endemic to Ghana. I am an intern, and therefore don’t have the confidence that comes with experience, so I must propose a differential diagnosis, because you cannot diagnose what you do not first think of. Here the differential would include other filarial infections like loa loa, lymphatic filariasis, or skin manifestations of a Treponema pallidum (syphilis) infection. However, if I was seeing this case in Duluth I would likely think of more common skin diseases depending on its appearance, such as lichen planus or perhaps just a hernia. When this day does arrive in Duluth, Minnesota and I am able to diagnose this because you all made me aware of it, you can count on me writing up a case report with a title similar to: “A rare case of onchocerciasis in Minne-Sowda.” (I hope you will describe this reference for the audience if I was correct). As for the other part of Dr. Naula’s case question regarding the confirmatory testing: it appears the standard test is a skin snip which would require a microscope. Again, if I am correct, my question for Dr. Griffin is if the dermatoscope that he speaks highly of could replace a microscope for this diagnosis in a resource limited clinic?
Thank you for all you do, and as I would say on the wards, strong work and godspeed.
Respectfully,
Jimmy
PS – For those interested, here is a photo from a rough day on the beautiful Lake Superior

James McCluskey III, MD
University of Nebraska Medical Center
Internal Medicine and Pediatrics – PGY1
Schuyler writes:
Good morning,
I hope all is well. I have been enjoying this case as it has led me to read quite a few interesting articles. Sadly, many of the things I read about didn’t align with the patient’s presentation. My original guess, infection with some sort of liver fluke (one of my all-time favorite parasites), made it into the short differential. Specifically, a liver fluke of the genus Fasciola. This is perhaps unlikely, as the patient had neither fever, nor jaundice, and palpable liver mass does not appear to be a common manifestation of infection. Definitely possible though – Samdanci et al. report two cases of Fascioliasis mimicking liver cancer in a 2019 paper*. I would recommend O&P or ultrasound to confirm diagnosis.
However, my money is on Cystic Echinococcosis (CE) because masses are more common in this disease AND because Dr. Naula said this patient does not have a TWiP ‘frequent flyer’. While I cannot recall any episodes about CE (though there may very well be some), I can definitely remember several episodes about liver flukes. Including the first episode I correctly guessed the Dx for (to myself of course, this was before I started writing in answers). Ultrasound or ELISA to confirm. Alternatively, examine farm soil or feces of the patient’s farm animals under microscope for eggs. I am not wholly confident in this diagnosis, as cysts evoke an image of being “fluid-filled” but the mass described in this case appeared to be solid. However, interesting as the parasite literature may be, I need to stop procrastinating and get back to studying and watching lectures.
Hoping for a book,
Schuyler (pronounced “Skyler”)
* https://pubmed.ncbi.nlm.nih.gov/28272650/
P.S. I would like to add one more diagnosis to the differential, though I’m unsure of how likely it is given the patient’s lack of symptoms: amebic liver abscess due to Entamoeba histolytica. I still think CE is most likely.
Alex writes:
Dear TWiP professors,
The ghanaian woman with the right upper quadrant tumor is probably infected with Echinococcus granulosus, one of the few parasitic cestodes infecting humans that I have the pleasure of sharing a habitat with. Since she lives in close contact with dogs and sheep, she was most likely infected by eating food contaminated with dog feces containing worm eggs. After ingestion, the eggs hatched and the resulting oncospheres migrated to the liver to form a hydatid cyst, which slowly grew larger and larger over time.
Since the medical team in this case is equipped for hernia surgery, I think it likely that they’d have an ultrasound device handy to take a peek at the cyst. Alternatively, it might be possible to identify the hooklets of Echinococcus in a sputum sample using conventional light microscopy. Less likely differentials include fasciolosis of the gallbladder and cysticercosis.
I would also like to comment on Dr. Griffin’s recent remark regarding your international audience being attributable to Prof. Despommiers “international appeal”. At the risk of sounding quite sappy, I want to say that to me, your appeal lies in the enormous amount of knowledge, interest and passion you all bring to this podcast. Educating others and sharing your experiences for the good of all mankind is obviously very important to you all and listening to your conversations really lifts my spirit during this damned pandemic. Thank you all, from the bottom of my heart. Stay safe and all the best to you,
Alexander
Foggy, 8°C/46 F and already dark outside at half past 4 here in Vienna
Martha writes:
Dear TWiP,
I was reminded to write by watching TWiN. My very short, short and long term memory is not what it once was. I sympathize with the mice. I was rather annoyed with myself for neglecting to write in regarding the prior TWiP since I had immediately guessed correctly that the agent was scabies.
This week’s problem is not at all in my wheelhouse and I had to scuttle around the interweb. To be very brief I am guessing: Echinococcus granulosus, causing a hydatid cyst from a dog tapeworm finding its way into the wrong host. I read that there is a reliable antibody serum test. But the way that the puzzle was posed, it seems that some other means of diagnosis was used. Since the clinic had surgeons and anesthesiologists, it would be possible to aspirate the cyst, obtaining hydatid sand and perhaps inner layer of cyst wall. Microscopy could show protoscoleces, which are the entities that would be the head of future tapeworms.
I have been enjoying all things TWI. Wishing you all the best.
sincerely Martha.
Marianne writes:
We are looking for a parasite which will cause a relatively large mass in the liver. Taken the lady works with sheep I think Echinococcus granulosus could be a plausible pathogen. Echinococcus is a cestode tapeworm which in intermediate hosts as humans and sheep cause cysts in liver, lungs or other organs. The definitive host (a dog) get infected when they ingest organs with cysts from the intermediate host. People get infected by hand-to-mouth transfer after taking care of their dog, dog poo, handling contaminated objects or ingesting contaminated water. I found out that the cyst may appear years after ingestion of the eggs and the cyst(s) itself may grow slowly over a long time and initially do not cause any symtoms. Over time though it may cause a mass effect in the organ it inhabits and depending of location cause symtoms. A bursting cyst may cause an allergic reaction.
Thank you for a great podcast!
Marianne Forsberg Ophthalmologist SWEDEN
Peter writes:
Hello dear TWIPpers and greetings from sunny Cape Town where the temperature is expected to climb into the mid 20s C today
The size and location of the swelling and mention of exposure to sheep has me thinking that the poor woman in Ghana has Echinococcosis. This is caused by the tapeworm Echinococcus granulosus. While the tapeworm in question often infects sheep (and goats), transmission to humans is normally via contact with the primary host, dogs [1]. After ingesting the tapeworm eggs the larva is released from the egg and penetrates the small intestine before reaching the liver via portal flow, where the metacestode implants, creating a hydatid (or fluid filled) cyst. The fact that cyst did not appear to be fluid filled suggests that it might have reached an inactive stage (stage CE4). Diagnosis is most commonly done using ultrasound [3] although serological tests are also an option (but perhaps not at this clinic). Treatment options depend on the stage of the cyst: in some cases PAIR (puncture, aspiration, injection of a scolicidal agent such as cetrimide, and re-aspiration) is used, in later stages a “wait and watch” approach is recommended.
The WHO reports that more than 1 million people live with this disease at any one time and that complications are common even after treatment. Prevention – through regular deworming of dogs and disposal of offal where dogs can’t eat it – is perhaps a better option than cure, but obviously not for this lady.
Peter
[1] http://www.wormboss.com.au/sheep-goats/worms/tapeworms/hydatids.php
[2] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4033287/
[3] https://www.who.int/news-room/fact-sheets/detail/echinococcosis
Brian writes:
Hello TwiP Team,
First-time guesser…
I believe the 50-year-old female was infected with Fasciola hepatica. F. hepatica can be found in its cyst form on the vegetation in areas where animal husbandry occurs and it was mentioned that the patient is a farmer who has sheep and goats. The metacercaria can be mistakenly ingested with watercress and subsequent hatching and migration of the trematode to liver occurs. F. hepatica infection is known to present as right upper quadrant pain, like the woman was experiencing. The solid mass mentioned in the case study could be an enlarged portion of the patient’s liver. An ELISA test can be used to determine if the patient has F. hepatica specific antibodies circulating in the blood.
Brian R.
*Response End*
Brian
Ph.D. Molecular Bioscience, Seton Hall University ’22
B.S. Biology, Monmouth University, ’18
Stacy writes:
Hi wondrous TWiPpers!
This is very exciting — my very first attempt to solve a case study. Having just read “Parasite Rex,” by Carl Zimmer and the “Parasite” trilogy by Mira Grant, my life is consumed by tapeworms. So, if I’ve made the wrong diagnosis, you’ll understand why.
My guess is that the woman from Ghana has a hydatid cyst caused by the “larval stage of Echinococcus granulosus, a tiny tapeworm (~2-7 millimeters in length) found in dogs (definitive host), sheep, cattle, goats, foxes, and pigs…” (CDC: https://www.cdc.gov/parasites/echinococcosis/gen_info/index.html).
The fluid in the cyst seems wrong, but wherever I looked, I kept coming up with ultrasound as a key diagnostic tool, so I am going to stick with my choice of cystic echinococcosis or hydatid disease. I looked up the availability of ultrasound in Ghana, and ended up reading an advertisement with the title: “Ultrasound Vital for Women’s Healthcare in Rural Ghana.” The highlighted case is of a woman presenting with “a very large mass in her abdomen.” The doctor’s fear is that it is “a malignancy of some sort.” But, using a portable ultrasound, she diagnoses the mass as a hydatid cyst. Obviously, an advertisement is no basis on which to make a diagnosis, but the similarity of case studies was interesting.
(https://www.sonosite.com/blog/ultrasound-vital-womens-healthcare-rural-ghana
I know that it is usually TWiV that accepts viewer recommendations, but I can’t resist making two here: The first is a YouTube series: “Journey to the Microcosmos.” (https://www.youtube.com/watch?v=kux1j1ccsgg&t=3s). Hank Green is the narrator and the sound track is by Andrew Huang. The second recommendation is Andrew Huang’s: “Peaches on Peaches”: (https://www.youtube.com/watch?v=C7NaFOBrhP8). I have loved both creators’ works separately for years, and having the two converge was a perfect moment for me.
Thank you for the wealth of knowledge that you impart. You push us all to be better people.
Stacy
Andrew writes:
Kia ora from Pongaroa,
Weather: a pleasant 18°C with a gentle rain that the local farmers will be loving.
Covid: New Zealand has had 560 fewer deaths, over the course of the pandemic, that would be expected. Births were also down go below the replacement rate.
Book: I am noticing that winners tend to be people who have not mentioned that they have not won yet so I am explicitly not going to mention that I have not won a book yet.
My guess for the well built lady from Ghana is a hydatid cyst caused by Echinococcus granulosus.
Reasons for:
- It is endemic in the area
- There are primary and intermediate hosts in the village – dogs and sheep
- There is a low-tech test available that can give a 90% accuracy for E. Granulosus infections affecting the liver. The Casoni test. The test involves an intradermal injection of sterilized fluid from a human cyst in one forearm and an equal volume of saline in the other forearm. Observations are made for the next 30 minutes and after 1 to 2 days. A wheal response with in 20 minutes is considered positive as is a reaction in 18 to 24 hours. The test is depreciated these days as it is only about 50% reliable in hydatid infections in parts of the body other than the liver.
- A search for hydatid cysts and E. Granulosus in the TWiP website gives just a few hits in the letters, as possible answers to cases, but none were a correct answer thus confirming Christina’s idea that it had not come up before in TWiP cases.
- The cysts are usually slow growing and often symptom-less which is why she might have thought she had a hernia.
Reasons against:
- the cysts are fluid filled and the examination indicated the lump was firm, floctuant and “did not appear to be fluid filled”. PD7 (p361) states that the liquid filled cysts are under pressure so may feel solid yet compressible when being palpated. If it is being held in place by plenty of adipose tissue a cyst might present like that. Also Dickson asked about how sure the non-liquid aspect was.I think he was also surmising E. granulosus.
So I will take a punt and stick with E. granulosus.
I have to say that I would love to see Christina on the show again even regularly as a co-host.
Mā te wā [mah tey wah] (see you later)
Andrew
Viki writes:
Good afternoon twipers! In remote Duluth MN, home of the world’s tallest infectious disease doctor and expert in Ehrlichiosis Johan Bakken, it is cloudy, 43 degrees by the lake and 40 degrees on the hill.
I’m going out on a limb here, because it’s fun. From https://www.reading.ac.uk/news-archive/press-releases/pr9938.html, I quote,”The placenta uses a cloaking device similar to that used by parasites to avoid detection by the mother’s immune system.” Could twip be having us on by playing with the parallels between pregnancy and a parasitic infestation?
So, I’m suggesting that the case of the woman with the growing lump in her abdomen, has an abdominal pregnancy. Her age seems to preclude pregnancy, and though being pregnant in one’s fifties is extremely rare, higher maternal age is also a risk for ectopic pregnancy.
The hint that one test solved the case suggests, of course, that the test is a pregnancy test.
Cheers, Viki
PS
My odd concern with Aander’s dog having a tapeworm is that those two daughters are my granddaughters. Maia is a sweet tolerant dog, and is unlikely to have fleas, because it’s just so darn cold here (and Frontline), and more importantly, that dog hunts.
Here, where Aanders did his residency, surgeons opened the head of a toddler who was having seizures, expecting to find a tumor. I don’t think Aanders was a resident at the time and I learned of this from someone else who shouldn’t have told me. They found tapeworm cysts. After cleaning up the vomit from a nurse, they closed. Treatment was to keep the toddler comfortable until he expired.
How did this child acquire the infestation?
V
Katy-Jane writes:
Dear all,
I am sitting in northcentral Wisconsin, where the weather is cloudy but a balmy (for this time of year) 55F/12C. (Long may it last!) I write regarding Christina’s case of the Ghanaian woman with a large swelling in right upper abdomen. The lump felt firm (not fluid-filled), the patient was not jaundiced, and appeared in good health.
My first two thoughts were schistosomiasis (S. mansoni) or malaria (Plasmodium falciparum). However, upon further reading, it seems that liver swelling tends to occur in advanced cases of these diseases, with fluid in the peritoneal cavity and diarrhea occurring in schistosomiasis and jaundice accompanying malaria.
Ruling those out, I returned to my old friend Google, which led me to cystic echinococcosis (E. granulosus) and fascioliasis (F. hepatica or F. gigantica). Both of these parasites can cause tumor-like symptoms in the liver and hang around sheep. I don’t have the best reasons for ruling out the liver flukes, but I think the symptoms have been around too long to be flukes, whose symptoms typically last a matter of weeks.
So I am going with E. granulosus as our culprit. The patient was surrounded by plenty of sheep and dogs, the intermediate and definitive hosts, respectively, for the parasite. The liver cysts can reach over 20cm in length. Development of cysts may take years, and calcification can occur, which could explain the reason the woman’s cysts were described as not feeling fluid-filled. According to PD7, “A definitive diagnosis can be made by microscopically identifying hooklets in sputum.” It seems feasible that this could be done in a remote area where other tests are not possible.
Thanks again for all your hard work!
Katy-Jane Shanak
Adjunct Faculty in Veterinary & Dairy Sciences
Northcentral Technical College
Wausau, WI
James writes:
RUQ mass in 3rd world farmer, seemed solid to physical exam.
In the third world, liver cancer (Hepatoma; hepatocellular carcinoma) is a leading cause of malignancy. It’s related to chronic hepatitis B, possibly aflatoxin.
Cholangiocarcinoma, carcinoma of bile ducts, is ALSO a problem and CAN be related to a parasite actually like Clonorchis that chronically irritates the bile ducts.
But I’m thinking that this case is pointing towards Echinococcus which is a tapeworm where WE are the accidental intermediate host. The cyst is lined by worm epithelium and buds off scolices (heads). Sometimes the cyst is full of so many worm heads that it can be called “hydatid sand.” I’m guessing it is very tense which is why it did not feel like fluid.
Having been on numerous medical mission trips, we almost always had an ultrasound with us. The later trips involved a small probe and an iPad; they have gotten very affordable.
We saw a few cases in Basque shepherds in Utah when I was a pathology resident and being such a Micro Geek I always loved them. Colorado is known for lamb and sheep, lots of Greek families ranch sheep up in the mountains, but I don’t recall seeing a case of Echinococcus here despite working in a liver transplant and care hospital. Legend has it that patients can get a lot of IgE to the worm and if the cyst is accidentally ruptured anaphylaxis may ensue.
| James M. Small, MD, PhD, FCAPAssociate Professor of Pathology and MicrobiologyClinical Career AdviserRocky Vista UniversityParker, CO 80134 |
UCLan Parasitology Club writes:
Good Afternoon TWIP Professors!
It’s cold and dull here at the University of Central Lancashire but, as always, your podcasts are keeping us busy! The Parasitology Club found this particular case tricky – there were so many possibilities so we had to narrow it down to our top 2.
A lot of parasites are known to cause liver abscess; however, we believe that the pesky parasite causing the large swelling seen in the Ghanaian women is Entamoeba histolytica. Amoebiasis is generally contracted through ingestion of contaminated water or food (Williams, 2017). The Ghanaian diet largely relies on starchy roots (cassava, yams), fruit (plantain) and cereals (maize, rice). Starchy roots and cereals still supply almost three quarters of the dietary energy and diversity of the diet remains low. Due to this background and her location, she is likely to be living in an area with low water quality and poor sanitary conditions. Furthermore, she is a subsistence farmer which means she will be in contact with soil and fertilisers (most likely made of faecal matter), and these are also routes of infection.
Infected people do not always become sick, which explains her lack of symptoms associated to this disease, i.e., loose faeces, stomach pain and cramping. Amoebic dysentery is a severe form of amebiasis and is associated with stomach pain, bloody stools and fever. It may be that she has experienced some of these symptoms in the past (as the swelling was reported to be growing steadily over time), or her body may have become used to the low-quality water and lack of sanitation.
E. histolytica rarely invades the liver and forms an abscess however, in a small number of instances, it has been shown to spread to other parts of the brain. Liver abscesses are generally soft and give under pressure, but in this case the swelling was hard. This may be due to the high amount of pus that has been allowed to accumulate over the past year. Ünal, et al., (2020) also describe Amoebic abscesses as oval or round shaped, and likely to be found near the liver capsule in the right lobe of the liver.
Another contender for this case is Toxocara visceral larva migrans (VLM). This is a syndrome caused by infection with migrating larvae of other kinds of parasites (CDC, 2019) Most people do not experience symptoms. People can be infected by accidentally ingesting Toxocara eggs through dirt (i.e., during farming etc). It can also damage tissues and organs, which may explain the liver swelling. This syndrome tends to occur in regions of poverty, where parasites are more common.
For example, in hot, humid regions where eggs can survive better in soil. Echinococcus granulosus 'hydatid cyst’ causes zoonotic disease following ingestion of tapeworm eggs excreted in faeces of infected dogs (Al-Khalidi et al. 2020). Sheep act as intermediate hosts. Infected patients can remain asymptomatic for years. The disease usually affects liver, with 70% of lesions found in this area. Cysts grow at quick rate, reaching very large sizes before they become evident.
Finally, Schistosomiasis is caused by parasitic worms when skin comes in contact with contaminated water. As with the previously mentioned parasites, many people do not develop any symptoms. Eggs usually travel to liver or intestine, leading to inflammation and scarring of these organs (CDC, 2018). There have been numerous occurrences of this parasite in Africa and surrounding areas.
Thanks again for the interesting podcasts, we will continue to solve each case as best we can in our efforts to win the book!
Stay safe,
Chelsea on behalf of the University of Central Lancashire Parasitology Club
Ashley writes:
Hello Drs. Racaniello, Despommier, Griffin, and Naula,
The 2023 Global Health Track at Western University of Health Sciences College of Osteopathic Medicine of the Pacific Northwest presents the following differential diagnosis for TWiP 189.
- Toxocara Canis – transmitted by dog, contaminated soil, hepatomegaly
- Echinococcus granulosus – could cause a firm liver cyst & as a farmer, patient is presumably in contact with animals (or their feces) quite frequently and could have contracted the ‘tapeworm’.
- Entamoeba histolytica – fecal matter water sources, liver abscess, aspirate or biopsy the liver abscess to see what is inside.
- Cystic echinococcosis – exposure to animal feces, patient grows tapeworm for many years
- Fascioliasis – latent and chronic phases of infiltration of the liver causing a necrotic lesion resembling a hepatocarcinoma.
- Echinococcus multilocularis – unlikely northern hemisphere, liver abscess
- Schistosomiasis – water contamination but low rates of liver abscess
Thank you all for reviewing our submissions.
-Branden, Kaya, Adrienne, Megan, Alec, Jameson, & Ashley
Ashley Levanduski, MPH, USN ENS, OMS II
United States Navy, Medical Corps
Western University of Health Sciences
College of Osteopathic Medicine of the Pacific Northwest
Kevin writes:
Dr Christina Naula’s case study
A middle-aged woman comes to the hernia clinic with an almost 8 inch right upper quadrant (liver) mass. Described as “not cystic” on physical exam, but one would have to be an astute examiner indeed to have this much faith in the fingertips. Suffice to say: she has a big painless lump in her abdomen. Fortunately, she is otherwise healthy.
The old medical saw is that the liver is the largest organ in the body (now deposed by the skin…but you know, the skin is no viscera)…The many non-parasitic disorders that might result in a solid or cystic liver mass are listed in the endnotes. Parasitic considerations below are erected as straw men to be knocked down before my final assessment:
•Protozoa: malaria and leishmania love the liver. But they don’t result in masses. Amoeba will follow below.
•Trematodes: fasciola loves the liver, but is a duct dweller, not a mass maker. Schistosoma likewise wreaks havoc in the liver via the upstream flow of ova which cause portal fibrosis (see a terminal curiosity for tangential non-sequiturs). Schisto liver masses I could not find in the literature.
•Nematodes: soil transmitted helminths such as strongyloides can invade the liver but no case reports of masses could be found. Likewise for visceral larval migrans (e.g. toxocara), no mass. I did find a case report (Pinilla 2001) of ascaris invasion of the liver resulting in a 6 cm abscess. Clonorchis: not really found much in Africa.
•Insects: I could locate no reports of myiasis related liver masses in humans. The closest was a 1981 report of invasion of a mare’s liver by Gasterophilus intestinalis.
A commonly heard query in clinic, “But Doc, what could it be?”
My two leading diagnoses in this case are amoebic abscess and hydatid disease. Liver abscess from Entamoeba histolytica is unlikely here since 90-93% of cases have symptoms of fever and abdominal pain. However, amoebic abscesses can be quite large: The 1923 edition of Manson’s Tropical Diseases says that they are “frequently as large or larger than a coco-nut.” In a brazen use of culinary comparisons this text goes on to say “multiple lesions usually attain the size of a filbert or an orange.” (see a Terminal Curiosity regarding medical analogies and metaphors).
My final diagnosis is a hepatic hydatid cyst from Echinococcus granulosus. These cysts can be quite large and are frequently asymptomatic (in one series 75% of cases were asymptomatic). Women are more frequently affected with hydatid disease (in some series in a 2:1 ratio). Regarding the comment that examiners of our patient discounted a cyst due to lack of fluctuance, Dame Sheila Sherlock says, “The tension in the cyst is high and fluctuation is never marked.” The weak point in my diagnosis concerns the paucity of epidemiological data on hydatidosis in West Africa. The disease has been described in Ghana but chiefly in sporadic case reports. I will omit discussion of diagnosis of treatment except to say that expectant management of this case of chronic hydatid cyst is probably a prudent strategy after the possibility of malignancy has been eliminated.
Welcome to your Glaswegian guest. I salute your global spread.
ENDNOTES
Big liver masses: differential diagnosis
simple benign cyst
hemangioma
hepatocellular carcinoma, cholangiocarcinoma, cystadenocarcinoma, metastases,
syphilitic gumma
tuberculosis
infectious : pyogenic, fungal
focal nodular hyperplasia
regenerative nodule
Caroli’s disease
RE: initial fears of hepatocellular carcinoma (HCC) in our case:
Tachi K, et al Hepatocellular carcinoma in Ghana: a retrospective analysis of a tertiary hospital data. Pan Afr Med J. 320;36:43. Published 2020 May 28. 194 HCC cases. Korle Bu Hospital Accra… 75% cases in patients with HBSAg positive, HCC – 6th most common cancer worldwide, biggest risk factor=chronic hepatitis B infection (HBV) estimated prevalence of chronic HBV in Ghana = 13%
Das AK. Hepatic and biliary ascariasis. J Glob Infect Dis. 2014;6(2):65-72. The clinical disease spectrum comprise of pulmonary, intestinal (including intestinal obstruction), appendicular, hepatobiliary and pancreatic ascariasis. However human ascariasis is silent in the majority of infected persons or only associated with vague abdominal symptoms. Hepatic abscess may be solitary or multiple and contains pus. There is tender hepatomegaly, high fever, intercostal tenderness and edema along with right hypochondrial pain. These abscesses may result from dead ova released by female worms migrating up the CBD, producing a granulomatous inflammatory reaction with subsequent breakdown with eosinophil infiltration. It may be commoner in children.
Pinilla AE, et al. Liver abscess caused by Ascaris lumbricoides: case report. Rev Inst Med Trop Sao Paulo. 2001 Nov-Dec;43(6):343-6. Case report, 54 y/o woman, 6 cm sono liver mass
Mimic of melanoma—-devious nematodes: Maier M,et al. Nematode infection of the liver mimicking metastasis of malignant melanoma. Liver Int. 2006 Aug;26(6):742-5. Background: The differential diagnoses of a circumscribed mass of the liver are varied. Especially if a malignant tumor, capable of setting metastases to the liver, is known in a patient’s medical history, there might be difficulties in differentiating the tumor’s entity. CASUISTRY: We report a case of a 40-year-old male with a history of malignant melanoma in whom follow-up investigations revealed a mass in the liver. (mass in this case was only 1.5cm diameter), no definite species identified but numerous morphologic observations pointing to helminth infection… (see A Terminal Curiosity below for discussion of the term ‘casuistry.’
Tadmor A, Perl S, Weinberg H. Infestation of a mare’s liver with Gasterophilus intestinalis. Vet Med Small Anim Clin. 1981 Jan;76(1):85-6.
Hesse AA, Nouri A, Hassan HS, Hashish AA. Parasitic infestations requiring surgical interventions. Semin Pediatr Surg. 2012 May;21(2):142-50.
Manson-Bahr, Philip, Manson’s Tropical Diseases, 7th edition, Cassell: London, 1923 (free at google.books.com)
RE: amoebic abscess: “When single the abscess sometimes attains a great size. Frequently it is as large as a coco-nut or even larger ; it has happened that the entire liver, with the exception of a narrow zone of hepatic tissue, has been converted into a huge abscess sac. When multiple the individual abscesses are generally smaller, ranging in size from a filbert to an orange.”
Disconnected notes on echinococcus disease:
•consider a calcified non-viable echinococcus hydatid
•hepatic hydatid cyst…frequently asymptomatic until large size is reached
•95% OF HUMAN cases of hydatid disease are due to E. granulosus (vs E. multilocularis)
from Up to Date:

Shelia Sherlock, Diseases of the Liver and Biliary System, 11th ed. Blackwell: Oxford. 2002 Sherlock on hepatic hydatids: “The uncomplicated hydatid cyst may be silent and found incidentally. It should be suspected if a rounded smooth swelling, continuous with the liver, is found in a patient who is not obviously ill. The only complaints may be a dull ache in the right upper quadrant and sometimes a feeling of abdominal distension. The tension in the cyst is high and fluctuation is never marked.
Angheben A, et al. Is there echinococcosis in West Africa? A refugee from Niger with a liver cyst. Parasit Vectors. 2017 May 11;10(1):232. Italian investigators who are studying tropical pathologies seen in the recent influx of West African immigrants and asylum seekers. Really a case report of human hepatic cystic echinococcosis. They lament the lack of rigorous epidemiological data on the prevalence of this disease in the sub-Saharan Africa
Pohnan R, Ryska M, Hytych V, Matej R, Hrabal P, Pudil J. Echinococcosis mimicking liver malignancy: A case report. Int J Surg Case Rep. 2017;36:55-58. 38 y/o woman with a liver mass = 13 cm x 10 cm. Lung nodules were also described
Wahlers K, et al. Cystic echinococcosis in sub-Saharan Africa. Lancet Infect Dis. 2012 Nov;12(11):871-80. At least 5 species of Echinococcus are described…Authors state that several East African surveys describe a predominance of women among echinococcus surgical cases….Though hydatid cysts can occur in any part of the body, the liver is most frequently affected.
Siracusano, Alessandra et al. “Human cystic echinococcosis: old problems and new perspectives.” Interdisciplinary perspectives on infectious diseases vol. 2009 (2009)
DeMarais P, Flaherty JP, Arnow PM. Echinococcal infection in a Ghanaian patient. Lancet. 1992 May 30;339(8805):1357-8. Case report from University of Chicago of a 30 y/o woman who lived her entire life in Ghana prior to emigrating to Chicago. The CDC (1992) told the authors that echinococcus had hitherto been undescribed from Ghana.
A TERMINAL CURIOSITY
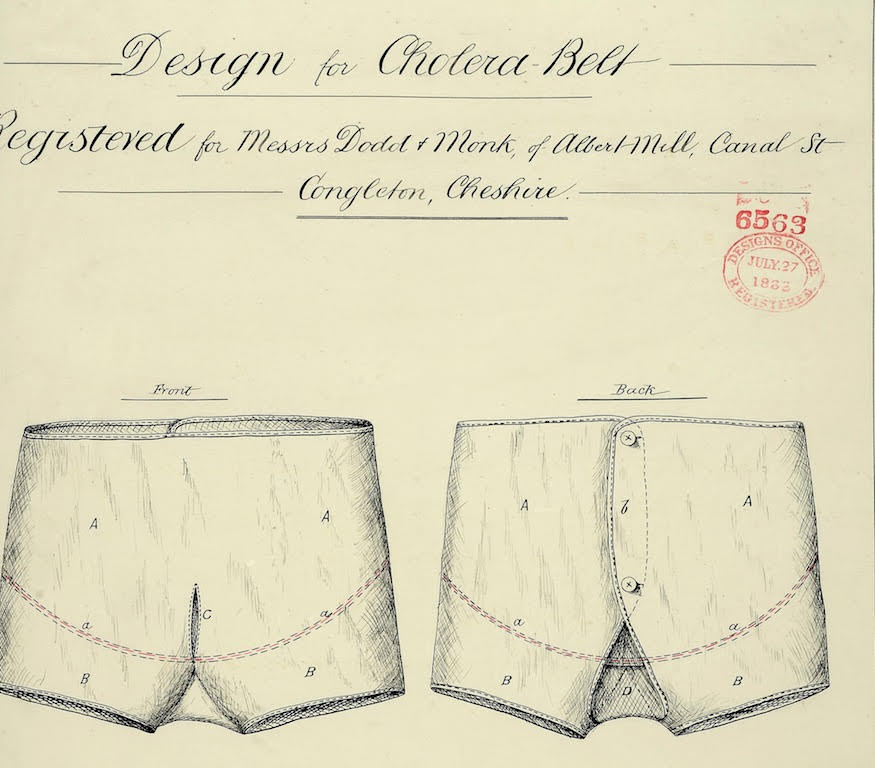
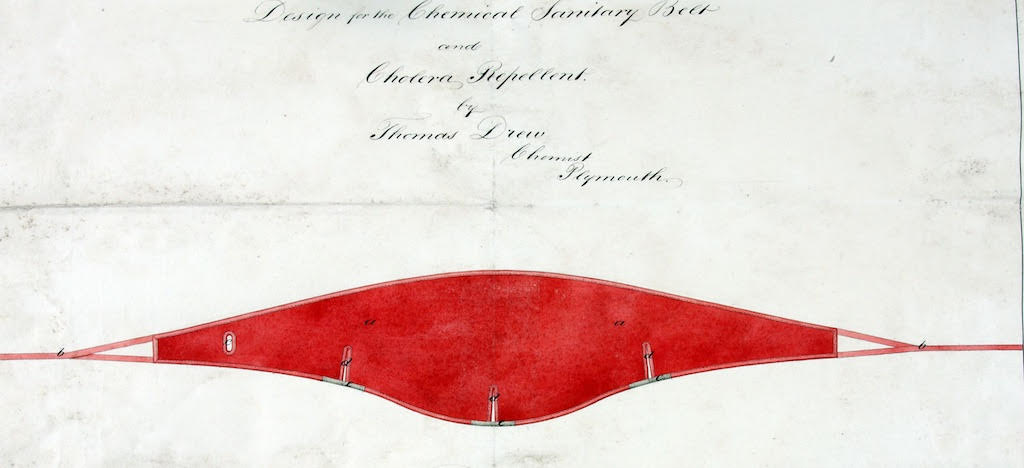
1. The Cholera Belt
In the very readable chapter on Tropical Liver in Manson-Bahr’s textbook, I came across mention of this hitherto (to me) unknown undergarment. Two versions are illustrated below. The cholera belt is part of a long tradition of binding and warming in medicine. The cholera belt began appearing in the medical literature in the mid-1800s. It was believed that insulating the abdomen from cold would somehow decrease the wearer’s susceptibility to cholera and other tropical liver and intestinal maladies. The whole story is exhaustively discussed by Renbourn: RENBOURN ET, The history of the flannel binder and cholera belt. Med Hist. 1957 Jul;1(3):211-25. (open access)
2. Symmers’ clay pipestem fibrosis

I’ve read about Symmers fibrosis in the past but my revelation while researching TWiP 189 was that the eponym here was not the possessive Symmer’s, but just plain Symmers. I always thought that there was an apostrophe in the term. Enough of that. William St. Claire Symmers was an English pathologist (1863-1937). He first described pipe-stem fibrosis in 1904 while working at the Kasr-El-Aini Hospital in Cairo. A further incidental: he was nominated for a Nobel Prize in medicine in 1937. If tobacciana isn’t your thing, I direct you to PIPEDIA, “a wiki for pipes” where the history of clay pipes is anatomized. This is unlikely to give the reader insight into the pathology of schistosoma induced hepatic disease, but it will give you some depth regarding medical analogies (see ref). Clay pipe use peaked in 1680-1700….snuff use caused a clay pipe decline 1720. Various resurgences followed, with an ultimate decline in use by the 1930s https://pipedia.org/wiki/A_Short_History_Of_Clay_Pipes
Pena GP, Andrade-Filho Jde S. Analogies in medicine: valuable for learning, reasoning, remembering and naming. Adv Health Sci Educ Theory Pract. 2010 Oct;15(4):609-19. doi: 10.1007/s10459-008-9126-2. Epub 2008 Jun 5.
3. Clay pipestems and metaphors in general
….prompts me to advise that the following terms be added to my list of culinary metaphors (TWiP 159), and flower, plant and vegetable metaphors (TWiP 172):
•Nutmeg liver
•Strawberry gallbladder
4. Casuistry
This word is always and probably unfairly linked with Jesuits. I was surprised to find it used in a medical context (see reference Maier M,et al. in ENDNOTES) Definition 2 in OED: A register or record of (medical) cases. 1883 J. W. Legg in St. Bartholomew’s Hosp. Rep. 19 202 Nor can I find any similar case in the casuistry of pemphigus as recorded in the year-books.
18 Caton writes:
Dear Twippers,
I awoke at 4 am this morning and was happy to discover that I had not yet listened to the Nov. 7, 2020 TWIP episode 189, Toe Jammin’, which entertained me until the “normal” waking hours. I was even more excited to hear the next mystery parasite clinical case, as I too, am a female farmer with who has goats and cows. And Dickson, I do wear shoes, usually boots, when tending to the livestock.
Upon hearing the clinical case, I immediately shouted out, “LIVER FLUKE!” (hopefully not so loud to awake other family members still sleeping). The clues were, 1) the location of the smooth mass just above the right side of the abdomen, which was thought to be liver cancer and 2) the definitive diagnostic test was done out in the bush, by doctors that only had equipment for their hernia practice. I figured they would have a dish and perhaps a microscope to do a stool test. I was unsure though, that a liver fluke could present as a gigantic palpable 22 cm mass protruding just north of her abdomen. Upon doing a little research I found the answer is yes, it could be.
“Fasciolosis is caused by the liver flukes Fasciola hepatica and Fasciola gigantica that are transmitted between mammalian hosts such as buffalo, cattle, sheep and other wild ruminants (or humans) as definitive hosts, and freshwater lymnaeid snails as intermediate hosts. In definite hosts, adult flukes reside in the bile ducts and the eggs are released into the environment through host faeces. Provided they come into contact with water, the unembryonated eggs develop further into miracidia, which hatch and infect aquatic snail as intermediate hosts. In the snail host the parasite eventually develops into cercariae before exiting to encyst on aquatic vegetation to form metacercariae. The cycle is complete when suitable definitive host ingest the infectious metacercariae on contaminated food substances or in water.”
Scientific African, Volume 8, July 2020, e00469
Prevalence of bovine fasciolosis from the Bolgatanga abattoir, Ghana
\FrancisAddyaKwameGyanaEnochArhinaMarionWassermannb
So, our lady farmer did not step in it, she imbibed it, likely at the same place she watered her livestock. Where animals drink, they also poop, thus passing whatever parasites they have into the water. Having been a Peace Corps volunteer for a couple of years, I know well that the majority of bush farmers do not have access to plumbing.
I suspect the fluke species was Fasciola gigantica not only because of the size of mass on her abdomen, but also because it is commonly found in the tropics and sub-tropics in Asia and Africa.
PS: I did my Peace Corps Jammin’ In Jamaica, 1991-1993. Yah, man. Lots of goats and bare feet. Luckily, also lots of stand pipes and water tanks.
Caton
S&C Nelson Farm, Grass-fed Beef
Iron River, MI
Jody writes:
Hi Docs,
I hope I’m not too late! I’m 4 for 4 now, and I don’t want to allow the elation I felt at my big win last episode to stop me from continuing my streak (or at least my pursuit) of diagnosis dominance.
On the topic of Christina from Glasgow’s case, a quick hunt for parasitic infections that might present as a mass in the neighborhood of our Ghanaian patient’s liver brought me to Entamoeba histolytica. According to PD7, hepatic amoebiasis can lead to tumor-like masses and pain and tenderness in the upper right quadrant of the abdomen.
Limited resources in the area the team was working in might not have allowed for ordering imaging or other advanced forms of testing, but microscopic examination of a stool sample might be possible, and may even allow for distinguishing between E. histolytica and E. dispar. Not sure if PCR machines are available but I would hope some lab optics would be on hand.
Another suspect is Oesophagostomum bifurcum, also endemic in Ghana and often presenting as an abdominal mass, sometimes asymptomatic, painless and hernia-mimicking. Fecal examination can again be useful for diagnosis.
And my word of the day after reading up on both of these is…coproculture. I will definitely do my best to work this into casual conversation in the coming weeks.
As always, stay safe and thanks for all you do!
Best,
Jody in Seattle
// L O S T L A B O R A T O R Y //
Srinivas writes:
Hello TWiPers,
I am new viewer of MicrobeTV. My interest in Microbe TV started towards the end of August with first watching TWiV and then slowly exploring other podcasts on the channel. I have sampled TWiEVO, IMMUNE and one previous episode of TWiP. There is plenty more to sample from —thanks to Dr. Vincent Racaniello — the host of all these wonderful shows.
I did a residency in Clinical Microbiology between 1981-84 in Puducherry, Southern India before moving to the USA for graduate studies in virology. I hope I still remember enough of the parasitology course I taught medical technology students then to hazard a guess.
A steadily growing mass associated with the liver in the upper right quadrant in Ghana in a subsistence farmer in her 50s. During the discussion of the case after the presentation, it was revealed that the farmer also owned sheep and dogs.
Could this be a case of hydatid cyst of the liver I wondered. I “DuckDuckGo”ed “Echinococcus granulosus” and read the available information on the CDC website and my suspicions were somewhat supported by what I gathered. I then dusted off my microbiology textbooks (Bailey & Scott’s Diagnostic Microbiology; Case Studies in Infectious Disease by Lydyard and coauthors, and Jawetz, Melnick and Adelberg’s Medical Microbiology) to gather additional facts and details.
Hydatid cyst of the liver (often in the lung as well) is caused by a cestode: Echinochoccus sps. The definitive host (where adult worms are present) is a canid (dog or fox). Both sheep and humans can be intermediate hosts (a dead end for the parasite for sure). The tapeworm resides in the small intestines of canids and embryonated eggs (oncospheres) are shed in the feces. When accidentally ingested by an intermediate host, the oncospheres hatch in the intestine and the larvae spread to the liver and lungs (sometimes brain or other organs) where they mature into cysts.
There are two species of Echinococcus: granulosus and multilocularis. We can rule out E. multilocularis as its primary host is the arctic fox and the disease is therefore restricted to the northern hemisphere. So my diagnosis would be hydatid disease due to E. granulosus. These cysts can grow quite large and if they don’t impinge on the bile ducts (biliary tree) there may be no symptoms of liver obstruction (e.g. jaundice). The cysts are thick walled and the fluid filled nature may not be discernible by clinical examination (e.g. shining a flashlight through it— this is usually done for tumors that reside just below the skin and easily accessible for such a test).
A CT or ultrasound would help in diagnosis by delineating the cystic nature of the lesion (thick-walled fluid-filled cysts with septa and sometimes floating septae resembling ‘water lily’) . Since the “mass” in the liver was identified by a team of surgeons there for hernia repair, it seems likely that some investigative tools such as ultrasound or mobile x-ray unit would be available. Ultrasound would be the one test to offer the patient. Although there is some disagreement as to which radiological test is superior, ultrasound or CT, CT would be less likely to be available there.
People develop allergy to the parasite. So a skin test with Echinococcus antigens is an alternative possibility. This is what we used to do during my residency. But I was never sure how the locally prepared antigens used for the test were standardized between different batches. Luckily the text books say that we now have serological assays (ELISA, indirect hemagglutination assays and latex agglutination assays). However, from the discussion, it is not clear if these serological tests are locally and/or readily available.
A definitive diagnosis will require an aspirate of the cyst contents and looking under the microscope for “hydatid sand” (protoscoleces and hooklets). Aspiration is fraught with the risk of anaphylaxis— it is therefore generally done during or after surgery (and very carefully!). There is also the risk of dispersing the protoscoleces during surgery resulting in more hydatid cysts in surrounding tissues and organs.
Having said that, one of the recommended treatments for hydatid cyst of the liver, when surgery is not an option, is PAIR (Puncture, Aspiration, Injection, Reaspiration). In this procedure, the fluid is aspirated (taking care not to leak any fluid into the surrounding tissues) and then the cyst is injected with ethanol to kill off the protoscoleces. The ethanol is then aspirated out after 20 minutes. An alternative way to kill the protoscoleces is by treatment with albendazole given for 1-3 months. This can be done prior to surgery or aspiration.
After writing the above, I was pleasantly surprised that I could freely download the PDF of “Parasitic Diseases” authored by Drs. Despommier, Griffin, Gwadz, Hotez and Knirsch from the Parasite Without Borders website. What a wonderful gesture and resource to the medical and scientific community! Thank you! The chapter on Juvenile Tapeworm Infection of Humans in this book provided encyclopedic details on hydatid disease of liver that seem to further support the initial diagnosis. According to what was written, ultrasound shows 90% sensitivity in diagnosis of hepatic hydatidosis.
I briefly also entertained amebic liver abscess and schistosomiasis (Schistosoma mansoni can affect the liver) as differential diagnoses. These diseases don’t present clinically in the manner described and were therefore not considered any further.
I look forward to listening to your next episode for the answer to this case study and to learn more about parasites!
Best wishes and regards
Srinivas
Crozet, VA