
Case guesses:
Josh writes:
Hi TWIP hosts
I’d like to thank you all for keeping us updated in the world of parasitology in these busy times.
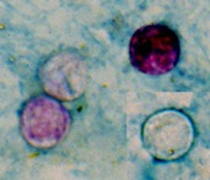
I’m excited to answer this case study as coming from South Africa myself. I believe the safari-goers have Cyclosporiasis caused by most likely ingesting contaminated food or drinking water containing sporolated oocysts of Cyclospora cayetanensis. My bet would be there is a food handler who is not engaging in good public hygiene practices .The giveaways where the frequency of the watery diarrhoea, typically 5-15 bowel movements a day, and Dr. Griffin’s emphasis on trimethoprim sulfamethoxazole, which is the 1st drug of choice. I’m assuming the GI PCR panel came back positive for Cyclospora cayetanensis and the good old Ziehl neelsen stain microscopy revealed the oocysts looking like this:
I’m hoping to go 3 for 3 in the latest case studies, interestingly the animal conservation and protection heavily relies on the tourism trade. The impact of COVID-19 is leading to a lack of revenue and funding to conservation efforts. Are we going to see an increase in poaching as nearby communities turn to it to obtain money in such a harsh economic climate? In order to help, they have recently implemented virtual safaris now… (https://www.andbeyond.com/bringing-africa-home/wildwatch-live/) I’m sure Dickson would like to enjoy a safari from the comfort of his living room at the fraction of the price….
On a side note, thank you Vincent for the virology lectures on YouTube and one lecture (#25) sparked my interest recently. You went onto explain prions and mentioned exotic ungulate encephalopathy can be found in Kudu… this sent me off to try and find out more about it. What interested me is that in South Africa we don’t seem to have any surveillance for it (I could be wrong). Many game farms have Kudu and they are bred as livestock as well, we also make biltong (what you refer to as jerky) with kudu. Would this be any worry or indicate a need for surveillance, are there any wild type prions (exotic ungulate encephalopathy) out there be transmitted across kudu similarly to the deer wasting disease crisis in the US? Sorry to go off track.
Thanks again TWIP hosts
Josh from Cape Town, South Africa
Dan writes:
Hello TWiP,
I’m back for my second guess. Using the MO of Ctrl+F’ing PD7 for “trimethoprim-sulfamethoxazole” brought me to Cyclospora cayetanensis as the most likely culprit.
Symptoms appear a week or two after infection (5 days is a little short), and include 5-15 watery bowel movements per day. Sensitivity of microscopic identification of the oocysts can be improved with acid-fast staining, which could explain why the first ONP without it came back negative.
Thanks for everything you guys do. You all are the heroes!
Dan
Heather writes:
Hello again my micro-friends! (Well, YOU aren’t small, but our shared interest in tiny pathogens is!)
I think the gentleman who travelled to South Africa has a cyclospora infection. According to the CDC, symptomatic patients may not shed enough oocytes in their stool to test positive from the standard stool culture/O&P, requiring the acid fast staining and PCR tests. My central deciding clue was that the zithro didn’t help him but Bactrim did. I suspect he got it from produce he ate on his fancy package deal trip since he was good about using bottled water.
I’m a frequent hiker and camper in the Blue Ridge/Smoky Mtns, so I’m familiar with giardia — but the zithro would have knocked that out if I’m not mistaken. And I don’t think the first round of doctors would have missed that common hiker’s foe!
I hope I’m right. I just discovered TWIP in the last month, and I’m less familiar with parasitic infections than other maladies. But if I’m not right, don’t worry. I’m not a doctor .
By the way, this morning when you read my pinworm letter first, you made my week! You guys are my close-second favorite public figures at the moment (second only to Dr. Fauci of course). My friends and family might be tired of me telling them what “Dr. Daniel” says is improving outcomes in COVID19 treatment, but that’s not going to stop me even once .
Stay well, from your favorite high school assistant principal,
Heather
Anthony writes:
I am writing in once again to provide my guess for TWIP case #183
The initial symptoms had made me think of Crypto, But the long duration and abdominal cramping coupled with the interesting find on the PCR panel immediately caused my mind to jump to Cystoisospora belli – a rather rare gastrointestinal infection but could perhaps be acquired in an area with rather poor sanitation!!!!
I think the fact that the patient recovered after a week of bactrim really cinched the diagnosis for me!
Keep up the amazing content!!!!
Anthony
Elise writes:
Dear TWIP Trifecta,
I do hope this finds all of you well. I was so pleased to hear that Dr. Racaniello remembered me, and I’m even more pleased to be writing back with a diagnosis guess for “Part 1” of the Two Part Case Study presented in TWIP 183.
I suspect the gentleman who went on safari in South Africa has been infected with cyclospora. The parasite is easily contracted via the fecal-oral route and given that the patient and his wife were traveling in circumstances where washing was unreliable, it sounds like the stage was perfectly set for an infection.
The symptom of frequent episodes of watery diarrhea, cramps and nausea is common to a lot of parasitic infections and I entertained a few other possible parasitic prime suspects like giardia, but the symptoms are somewhat different (the diarrhea in giardia cases is fatty and greasy versus the watery variety that the patient experienced).
Cyclosproa seemed like a more likely parasitic culprit for several reasons. First, the gentleman’s symptoms are most consistent. Secondly, he responded entirely favorably to the trimethoprim sulfamethoxazole treatment, which is a standard recommendation for treating cyclospora. And finally, his initial stool culture was negative. This is not uncommon with cyclospora infections and, one recommendation is to do multiple stool tests over a number of days, or alternatively, doing the additional tests that Dr. Griffin’s patient had done (ONP acid fast stain, GI PCR panel) .
I’m now extremely intrigued to see how the patient’s wife managed to get herself an entirely different parasite.
I appreciated this case because I have been traveling virtually and watching these daily safaris in South Africa on Wild Earth. Here is a link if you, too, want to safari vicariously, with no risk of parasites (at midnight or 9:30 in the morning Eastern Standard Time) https://wildearth.tv/safarilive/
It was sunny and about 63 degrees F (17 C) today in Lower Manhattan.
Again, I am so grateful to all of you. Big best wishes
Elise
Sophia writes:
Dear dedicated doctors! (as per the italian dottore). I hope I make Daniel proud this time (I guess he really wants us to learn this stuff!–Ancient Greeks said “repetition is the mother of knowledge”) so I will say the symptoms are due to Cyclospora cayetanensis.
Of course I cheated by looking at other twips and Kevin’s notes, who already has an A on this course and is just auditing for fun. I don’t think I will ever remember this organism. Anyhow, I do have a question: if you’re out travelling and you get infected with cyclospora, will the symptoms eventually resolve without any treatment or is it the case that you really need medication to get rid of this? I usually take immodium pills with me to stop the diarrhea but this won’t stop the organism from multiplying.
Thank you for making time for twip and happy birthday to Dickson!
Sophia, Greece, 35 degrees C due to sand storms from the Sahara (unusual for this time of year but what’s not unusual this year?)
Alexander writes:
Dear Professors,
it is 24°C / 75 F out today and it’s just now starting to feel like early summer is just around the corner. I’m a med student in Vienna, Austria currently working as a study coordinator for a COVID-19 trial.
I’ve lately been skipping all of the podcasts in my subscription list that even referenced that damn virus, with you and Christian Drostens works being the only exceptions. This has given me the opportunity to explore all of your other series, and having only been a regular listener of TWiV and TWiM, discovering TWiP was a special treat in this situation. Over the last couple of days I’ve binged your most recent episodes and listening to your case of the safari tourist immediately rang a bell for me.
The water shortage in the area of the resort they were staying in might be the primary cause here. While they felt they were safe drinking bottled water only, the kitchen might have skipped the washing of fresh produce, resulting in the transmission of the pathogen in question. The high frequency of diarrhea, the lack of fever, blood or steatorrhea and the response to trimethoprim sulfamethoxazole all remind me of the two volunteers in Uganda a few episodes back. This of course makes infection with Cyclosporidium cayetanensis the most likely diagnosis. This pesky fiend is endemic in South Africa where a large proportion of the vulnerable population is also at risk for complicated disease due to the high prevalence of HIV infection.
Isospora belli might cause similar symptoms but has a longer incubation period of 7 to 10 days and required a more prolonged therapy.
Blastocystis hominis might also be the culprit, but it’s role in pathogenesis remains controversial. Anyways, seeing as I have no experience in the field of parasitology except for listening to your podcasts, I might be the victim of the famous Dunning-Kruger-effect here.
I really enjoy everything you produce at microbe.tv. In these stressful times, they are a cherished reminder of what I want to do as a doctor and what I’m passionate about. I’m looking forwards to all future episodes of TWiP and the other Twi’ses and I hope you’re all staying healthy and looking out for yourselves. Best regards,
Alexander, Vienna
Cecelia writes:
Dear Doctors,
I think your 70 year old patient returning from South Africa has Cyclospora cayatanensis. His frequent diarrhea, nausea, and abdominal cramping are consistent with the symptoms. The fact that he was staying in an area with severe water shortage made good hand hygiene almost impossible.
Another factor is that C. cayatanensis
is endemic in many parts of the world making it easier to become infected from contaminated food and water.
I did consider the cause of his diarrhea could be from Cystoisospora belli, because it is also diagnosed with a modified acid fast
stain and treated with trimethoprim sulfamethoxazole.
However I ruled out C. belli because there was no mention of fever in the patient and C. belli infection is much less common.
Thanks again for your great podcast.
Sincerely,
Cecelia
St. Petersburg, Fl
Kush & Karishma write:
Dear Twipanosomes!
I’m writing in to you from Birmingham, England where it’s currently 19degrees celsius and sunny with a cool breeze. My wife and I are both physicians in training and have been listeners to your fantastic podcasts for a few years now, but have only just mustered up the courage to email in our thoughts on the case study.
The clinical presentation of watery diarrhoea in returning travellers of course has a very wide differential diagnosis, so it was the need for an acid fast stain and treatment with co-trimoxazole that narrowed it down.
As far as I know the acid fast stain is used on stool to identify either cryptosporidium, cyclospora or cystoisospora. All of these can be a cause of watery diarrhoea, but cryptosporidium is treated with nitazoxanide (or in HIV patients with HAART), whereas co-trimoxazole is an effective treatment for both cyclospora and cystoisospora.
As the diarrhoea has been going on for two weeks in an immunocompetent individual we reckon the most likely diagnosis here will be cyclospora,
Thank you for the awesome podcast, keep up the good work!
Kush & Karishma
James writes:
My wife and I are going on a TWIP soon to see our daughter, grands, and son in law in Tennessee. It is freaking arthropod central down there, ticks, chiggers, skeeters, you name it.
Anyway, 70 year old dude goes to South Africa and gets watery diarrhea for two weeks. A bit long for E. coli or most viruses and after all this IS TWIP.
Regular O and P is negative but Acid Fast O and P is positive. This is a modification of the Acid Fast stain used for mycobacteria, and it stains the oocysts of the Big three C’s: Cryptosporidium, Cyclospora, and Cytoisospora. Used to be Isospora as I recall. The oocysts of Cryptosporidium are somewhat smaller than those of the other two (my medical students actually knew that a couple of weeks ago for their parasite quiz) and also are susceptible to Septra/Bactrim/Trimethoprim Sulfa. I’m not certain that we have enough to distinguish between C. belli and C. cayatensis here but, who cares?
My PhD half cares but my MD half doesn’t.
I did diagnose a few of these coccidians on small bowel biopsies back in my active pathologist days. Oh, you’ll like this, I also diagnosed two cases of Whipples and we even did EM on the biopsy.
The San Francisco HIV site says that Cryptosporidium is 4-6 microns, about the size of a Candida yeast. Cyclospora is about twice that and Cytoisopora is up to 25 microns, but I’m sure there are better molecular tests out there in countries that can afford them!
Teaching is interesting with Zoom, recorded powerpoints, email, and message boards but so far so good–got excellent reviews for the Microbiology course this year, taught from my stand-up desk in the corner of my home office. It’s looking like most of my work will be done here at least until January and possibly NEXT June.
TWIP on dudes.
| James M. Small, MD, PhD, FCAPAssociate Professor of Pathology and MicrobiologyRocky Vista University |
Andrew writes:
Kia ora to Grumpy, Sleepy and Doc from Pongaroa
(In my opinion Dixon should be called Happy because he tells the best jokes, but it is his choice.)
No book won yet – but that is OK, I am secretly waiting for the 8th edition
Weather is 16°C and raining
Covid-19:
We are now in level 2 and we have just 27 active cases (down from 929) and country wide travel is now allowed but social gatherings are limited to 100 people with exceptions for some funerals due to cultural factors. Schools are open as are restaurants and bars. These restrictions led to our Prime Minister and her family being denied access to a popular café. The happy end was that a table freed up and a staff member raced down the road to inform her she could come in.
Public transport and shops are required to maintain the 2 meter social distancing but masks are not required. The borders remain closed to all non-citizens. There is talk of establishing open borders with other countries that have or will soon achieve zero community transmission. This will be important for our tourist industry and curiously people waiting for overseas post; many countries cannot send us mail due to the lack of aircraft flying to and from our shores. One of many third order consequences of the pandemic. The ramifications of the pandemic will last well into the coming decades and I hope that we will use mountains of data collected to prepare for the next pandemic whatever the pathogen is; viral, bacterial, or parasitic.
My guess for the man who holidayed in a drought-stricken South Africa and was suffering form diarrhea:
As I see it, there is not enough information to determine which parasite was in play, even if I rule out those relying on insect vectors because of the dry conditions. I am thinking the wife’s symptoms might make it clear which organism was responsible and that being the reason Daniel has a sequel to this case – TWIP 184. I made a table and checked off those parasites left against the symptoms, geographic spread, transmission route, tests and treatment. The idea being to allocate a probability to each. The surprising factor, for me, that limited the selection the most was the successful treatment with TMP-SMX. So my Bayesian priors are:
Cyclospora cayetanensis 55%
Cystoisospora belli 25%
Blastocystis hominis 10%
Something else 10%
I am really looking forward to the denouement.
Ngā mihi,
Andrew
Jim writes:
Greetings distinguished antagonists of the viral misinformation:
Sometimes people who travel abroad to see exotic wildlife, will encounter more creatures than meet the eye.
In this case, the two patients were probably infected, Via the fecal-oral highway, with the parasite Cyclospora which they might have contracted while eating at the lodge.
The water shortage could have adversely affected normal standards of uncooked food preparation in addition to fostering poor hand hygiene.
As we learned in an earlier TWIP released around the dawn of the Covid-19 era, the medication known as Bactrim should be effective against this protozoan parasite.
Many thanks to the three of you for your continued leadership on TWIP and TWIV and especially to Vincent for all of the other podcasts in the TWIx universe. You guys are making a real difference. I would urge all those who have not yet contributed to add their support through Patreon.
Take care, be safe and remain humble,
TWIP rocks the roiling ‘20s!
Jim
Bethany writes:
Hello!
I’m a relatively new listener and first time case-study respondent. I was a few episodes behind because I’ve been trying to keep up on all of the wonderful TWiV episodes released, but I finally binge-listened to a bunch today. Lucky for me, I think the diagnosis for this case is the same as episode 181- cyclospora cayetanensis!
Over 10 episodes of watery diarrhea and resolution after Bactrim treatment were the main clues for me. I don’t know if this email is too late or if you read all of the emails you receive, but as a PhD student in infectious disease, I would love to expand my infectious agent text book repertoire!
Thank you for all you do!
Fauci for President!
Regards,
Bethany
University of Central Lancashire Parasitology Club writes:
Dear TWIP Professors,
Hello again from the Parasitology Club at the University of Central Lancashire in the beautiful North West of England.
This strange semester is more or less over having switched to on-line teaching and examinations in March due to COVID-19 restrictions. Marking of assignments and exams has been completed so the summer has started for students and planning for next semester has started for staff and we have beautiful weather to cheer our spirits further.
The case of the gentleman of three score years and ten, returning with his wife from South Africa with more water in his stool than was available for handwashing on his African sojourn.
The profuse diarrhoea, nausea and abdominal cramping would suggest enteritis and without the narrowing of the field to parasitology could suggest an infection with a toxigenic E.coli, Campylobacter jejuni, Salmonella or other enteric bacterial pathogen due to poor hygiene in food preparation or inadequate water treatment. The negative stool culture directs us to another likely cause.
Two of the most common parasites associated with diarrhoea would be Cryptosporidium and Giardia.
Giardia is relatively easy to detect in stool with transmitted light microscopy although shedding of cysts can be intermittent in and could explain the negative OCP result, but the symptoms are not typical of the foul smelling, fatty, floating stools we rarely relish to examine for Giardia.
Three coccidian parasites could be the cause of these post-vacational sequelae; Cryptosporidium parvum, Cystoisospora belli and Cyclospora cayetanensis. All three stain well with acid fast staining techniques which are necessary to improve the microscopic detection of these smaller and less structurally distinct organisms.
An auramine stained smear positive for Cryptosporidium oocysts, examined under UV illumination is a thing of beauty and could have been a likely explanation for the frequent evacuations of this septuagenarian pair, however this infection is not treatable with sulphamethoxazole-trimethprim combination drugs and so would not fit the pattern with the resolution which seems to be associated with treatment. Cryptosporidiosis in the immunocompetent individual should normally resolve within 7-10 days and there is no suggestion in the notes that the unconstipated couple are immunosuppressed in any way.
This leaves us with the two coccidians that could cause these symptoms and are both more common in the tropics and sub-tropical areas of the world. Both these agents will respond to treatment with the drugs prescribed and are transmitted through food and water where good hygiene is difficult to achieve.
Cystoisospora belli infection is reported to be associated mainly with immunocompromised individuals and is considered to be rare. Cyclospora cayetanensis is becoming more frequently encountered and associated with travellers’ diarrhoea and outbreaks particularly associated with soft fruit berries. This epidemiology of this organism suggests that humans are the main host and perhaps the poor hygiene in camp resulted in the sharing of more than bon appetite, during meals.
Without more details of the acid fast microscopy we will place our chips on the likely cause to be Cyclospora cayetanensis.
Thank you as always for your wonderful podcasts and stimulating case studies.
David
On behalf of the University of Central Lancashire Parasitology Club
Dr David Wareing
Lecturer in Medical Microbiology
University of Central Lancashire
Chris writes:
Good morning Docs,
it is a beautiful 70~F day here in stony brook Long Island with sunny skies all around. First I would like to start this email by saying thank you to all three of the TWIPsters, as your continued persistence through this pandemic has been greatly appreciated and informative. Now for my case guess, I believe the patient is suffering from Cystoisospora belli a protozoan parasite that lives in the intestines of people and is known to cause watery diarrhea. This parasite is typically well tolerated by most people but is of great concern if you are immunosuppressed and has caused serious illness for many HIV/AIDS patients. This parasite is normally transmitted through the fecal oral route and is best avoided through proper food handling and general hygiene (I.e thorough hand washing).
Attached below is a new article from a little while ago about the Peconic bay scallop die off that occured this year. The die off revealed the presence of a Apicomplexan parasite heavily infecting the kidney of these animals( discovered by the Marine Animal Disease Laboratory at Stonybrook) . The heavy infection in addition to warm waters with low oxygen is believed to have caused the massive die off. Thought it would be interesting to share so local parasite news. https://suffolktimes.timesreview.com/2020/02/parasite-linked-to-scallops-die-off-in-peconic-bay-dec-says/
Another topic of possible interest is an observation I have made over the last year concerning parasites of horseshoe crabs. Dickson likes to say that “successful systems attract parasites”, which I fully agree with. However Horseshoe crabs, a species that is ~450 million years old, is surprisingly not host to many parasites. there is a scarcity of information on the topic with the last papers addressing Horseshoe crab parasites from the 60s. From my own personal necropsies and Literature review I have gathered that there is only 1 trematode species that infects these dinosaurs, a metacercaria ( Microphallus limuli), 2 nematodes ( Monhysteria spp. and Grathponema sp) of which I have only observed 1, a few protozoans (not very well investigated so probably underreported) and a handful of triclad turbellarian worms however these are still commonly referred to as commensalist. Just an interesting observation that such a stable host (arguably one of the most stable) has a relatively small amount of parasites communtiy, also I thought Dickson might enjoy the observation as he is a fan of both parasites and has mentioned he is fascinated by horseshoe crabs.
Lastly, I would like to point out that Springer recently made a few hundred textbooks free online on topics from all disciplines So I thought the TWIP listeners might enjoy the link. I’ve already picked up 2 books on survival analysis.
Once again thanks for everything and stay safe!
warm regards,
Chris
P.S
I put this last bit as a post script as it may be off topic, so feel free to ignore if thats the case. Y’all have mentioned how viruses are parasites so I thought it could be appropriate and a nice break from COVID-19 discussion. In aquaculture a common technique utilized around the world is triploidization, in which hatchery raised animals are bred to have an extra set of chromosomes. This is commonly done to sterilize the animals for both Bivalves(1) and fish(2) and can increase yield for certain species (3). So the question I have for Vincent is, how do you think that these animals would respond to viral infections, from a theoretical standpoint, being that they have 1.5x the amount of DNA than their diploid counterparts. There are a few studies looking at how Viruses of these animals impact survival, however most of these studies (4) don’t address the cell biology of the virus, just the results of infection(survival). So i’m curious to hear what a virologist would think about how this fundamental change in the cell would influence a viral infection.
JHS3W83XryiB2OzmOLteCUol5ejE3eq-xhZyxICCK7ZT7_WzwKww-L-zg
2)https://link.springer.com/article/10.1007/s11160-004-8361-8
4)https://www.int-res.com/abstracts/aei/v2/n3/p215-237/ there are more sources but I imagine you are too busy to read through a bunch of papers on fish and oysters
—
Christopher Brianik
School of Marine and Atmospheric Sciences,
Stony Brook University, Stony Brook, NY
Kevin writes:
Safari guy done got the flux.
What’s this whole world comin’ to
Things just ain’t the same
Any time the hunter gets captured by the game
(1966 song by The Marvelettes )
This case has some ironic asymmetries. As a consequence of visiting the largest herbivores and predators on earth, our patient’s intestine has become the destination of a microscopic tourist. And, apropos of nothing in particular, I’m reminded of a popular T-shirt trope from the recent past: My parents went on safari and all I got was this lousy protozoan….
This case shouldn’t be regarded as a re-run, despite the culprit’s appearance in TWiP 180. I say this because Cyclospora is something of a newcomer to the table, having been definitively described in 1993. Some relevant tidbits follow—-
- Cyclospora cayetanensis, a coccidian protozoan parasite. No known animal reservoir. No experimental animal model. Worldwide distribution.
- Incubation period averages 1 week (range, 2 days to ≥2 weeks). Fits well with our case.
- Clinical descriptions highlight the VOLUMINOUS and watery nature of the diarrhea
- Diarrhea can be profuse, can last weeks to months and may be remitting and relapsing
- source of infection is consumption of contaminated food but water-born and soil-born infection also occur.
- Various fresh fruits and vegetables are frequent sources (berries and leafy greens–presumably due to the difficulty of cleaning these thoroughly).
- North American outbreaks frequently cite raspberries and cilantro.
- Uncommon/rare post-infectious syndromes such as Guillain-Barre and reactive arthritis.
- Diagnosis most reliably via nucleic acid multiplex-array testing such as BioFire assay, outperforms microscopy (eg wet smears, acid-fast staining.
- TMP/SMX is the antibiotic of choice, tho can use cipro in sulfa allergic patients. Nitazoxanide has also been used.
- CDC ‘Yellow Book’ 2020: “The risk for Cyclospora is highly geographic and seasonal: the most well- known risks are in Nepal, Peru, Haiti, and Guatemala.”
Prevention should have been the best policy, but being on safari in the middle of a water shortage has some drawbacks. Fortunately our adventurer didn’t seem to pick up any other diseases.
TWiP 3-sum: hardest workin’ guys in New Yawk, how do ya fig-ya ??
ENDNOTES AND REFERENCES:
Ortega YR, Sterling CR, Gilman RH, Cama VA, Díaz F. Cyclospora species–a new protozoan pathogen of humans. N Engl J Med. 1993;328(18):1308‐1312 The article that is the first official description of this “new” disease agent.
Almeria S, Cinar HN, Dubey JP. Cyclospora cayetanensis and Cyclosporiasis: An Update. Microorganisms. 2019;7(9):317. Published 2019 Sep 4 A very comprehensive and readable review.
McHardy IH, Wu M, Shimizu-Cohen R, Couturier MR, Humphries RM. Detection of intestinal protozoa in the clinical laboratory. J Clin Microbiol. 2014;52(3):712‐720. doi:10.1128/JCM.02877-13 OPEN ACCESS
Giangaspero A, Gasser RB. Human cyclosporiasis. Lancet Infect Dis. 2019;19(7):e226‐e236. doi:10.1016/S1473-3099(18)30789-8
Chacín-Bonilla L. Epidemiology of Cyclospora cayetanensis: A review focusing in endemic areas. Acta Trop. 2010;115(3):181‐193
Markus, M. B., and J. A. Frean. 1993. Occurrence of human Cyclospora infection in sub-Saharan Africa. S. Afr. Med. J. 83:862-863.
A 2010 review of global epidemiology of cyclospora—22 countries surveyed….average estimated infection rate of 1.7%.in approx 47,600 immunocompetent patients most attending clinic with diarrhea complaint… …a 2011 metaanalysis of sub Saharan African patients reported an overall prevalance rate of 18%
Fletcher SM, Stark D, Ellis J. Prevalence of gastrointestinal pathogens in Sub-Saharan Africa: systematic review and meta-analysis. J Public Health Afr. 2011;2(2):e30. Published 2011 Sep 5.
A summary of 27 studies. Cyclospora was isolated in 18% of clinical samples…
It can be safely said that the infection is not uncommon, ranging from endemic prevalences from 0.6 to 24% in a variety of worldwide studies….
CDC Domestically Acquired Cases of Cyclosporiasis — United States, May–August 2019
Last Updated NOVEMBER 19, 2019 4:00 PM EDT
https://www.cdc.gov/parasites/cyclosporiasis/outbreaks/2019/a-050119/index.html
Something to look forward to: domestically acquired cyclospora is most common in spring and summer.
“As of November 13, 2019, 2,408 laboratory-confirmed cases of cyclosporiasis were reported to CDC by 37 states…144 hospitalized. 10% cases were linked to fresh basil imported from Mexico. Increase in cases compared to previous years is attributed to the increased use of multiplex GI diagnostic panels”
Picture THIS:
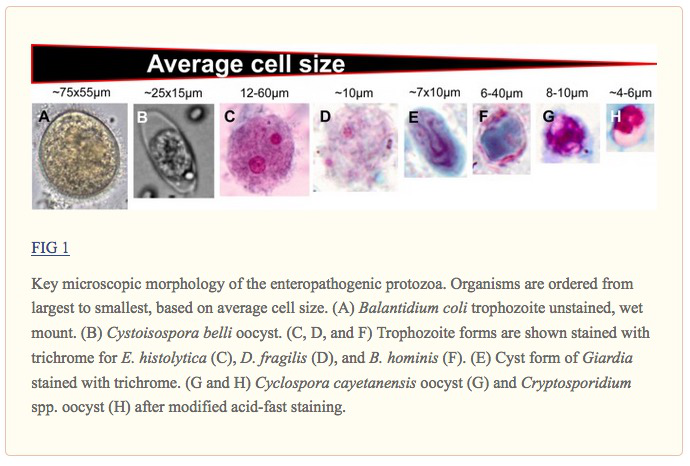
Illustration from McHardy et al 2014 (OPEN ACCESS)
A TERMINAL CURIOSITY
Attempting to remain fashionable in plague-time, and trying to stray from the classics like DeFoe and Camus, I read through Richard Mead’s A Short Discourse Concerning Pestilential Contagion, and the Methods Used to Prevent It 1720. I highly recommend this short and delightful essay. Though often suffering from many 18th Century erroneous medical theories, The Short Discourse contains many items that have a distinctly current ring to them. A passage that I found particularly relevant:
“…leaving the place infected is the surest preservative, so the next to it, is to avoid, as much as may be, the near approach to the sick, or to such as have but lately recovered. For the greater security herein, it will be advisable to avoid all crowds of people. Nay it should be the care of the magistrate to prohibit all unnecessary assemblies, and likewise to oblige all, who get over the disease, to confine themselves for some time, before they appear abroad.”
By the way, Mead also contributed some observations on our faithful pal, Sarcoptes scabei:

Martin writes:
Dear fellow parasite enthusiasts!
I am an equine parasitologist at the University of Kentucky, and I have been a steady listener to your podcast for several years now. Yes, horses get lots of parasites, and we sure have lots of horses here in the horse capital of the world. I enjoy your podcast as it makes a perfect soundtrack for jogging around the neighborhood, and it provides great material for discussions with my students. I appreciated your discussion of the hidden antigen vaccine for Haemonchus contortus in your last episode as it is close to home for me (I will refrain from lecturing Dickson on how to pronounce abomAsum, as I am sure others have done so already). I dabble a little with science communication myself, and have launched a video series on the parasites a horse encounters in its life – in the order of appearance. The videos are posting once a week on our Facebook page (https://www.facebook.com/GluckEquineResearchCenter/ ), and have been well received here during the global COVID-19 shut-down. You can also find the videos on my YouTube Channel:https://www.youtube.com/channel/UC_pDqB6sRvi1XJ8AHUapPCw?view_as=subscriber .
Anyway, I am writing to you as I have a nomination for your parasitology hero segment. Dr. Eugene T. Lyons is a legend in equine and sea mammal parasitology. He was the first to describe a lactogenic route of transmission of a nematode parasite, which was considered unlikely, if not impossible at the time. He first unraveled the life cycle of the hookworm of Northern Fur Seals, Uncinaria lucasi, and demonstrated how larvae were passed from mother seal to her pups through the colostrum. Then, he went on to demonstrate lactogenic transmission of Strongyloides westeri larvae in horses. He worked here at the University of Kentucky for 56 years and has published over 300 peer-reviewed scientific papers. His contributions also include work on life-cycles of other important parasites in horses as well as pioneering drug discovery and testing. And he was instrumental in documenting drug resistance in important equine parasites. He worked seven days a week, year-round and the only vacation he ever took was to participate in field trips studying parasites of his beloved seals and sea lions. His day would start at 6am in the morning, and he would continue until evening time – every single day. I had the fortune to work with him and learn from him for several years before his passing in December, 2017. He was humble but generous with his knowledge. And he enjoyed interaction with young people, teaching future generations of parasitologists. You can read more about him in the In Memoriam piece (attached) that I wrote for him and his technician, Sharon Tolliver, who were inseparable for over 45 years of working together and passed away just a couple months apart. I also enclose his publication list and a few pictures of him.
Please let me know if you need anything else. I truly hope that you will extend this honor of adding Dr. Lyons to your list of parasitology heroes.
Sincerely,
Martin K. Nielsen
DVM, PhD, DipEVPC, DipACVM
Co-Editor-in-Chief, Veterinary Parasitology
Associate professor
Schlaikjer Professor in Equine Infectious Disease
Department of Veterinary Science
M.H. Gluck Equine Research Center
University of Kentucky
Lexington, Kentucky