
Case guesses:
Sophia writes:
Hello professors
this will be short as I am writing this in a rush: I would say, if it’s not malaria (first smear negative but how about a 2nd one?) then it is leishmania. Or I could be wrong.
Incidentally, question for Dr. Griffin, speaking of limited resource settings when are RDTs for malaria used instead of the smears and how reliable are they? Do you do them at all? apparently there is a mutation in the population in some countries which renders these tests quite unreliable.
Just wondering…
Here’s to another year of podcasting and more cases….
all the best to you and thank you for doing this
Sophia, Greece, 0 degrees C
Peter writes:
Dear Doctors,
Having thought about this case study I believe that a reasonable guess that appears to fit the geographic location and patient symptoms is schistosomiasis, a parasitic disease caused by trematode worms of the genus Schistosoma. This case appears to be a recent acute infection, since symptoms only began a few days ago. The diagnosis is supported by the facts of the girls recent poor health, particularly her enlarged and sensitive spleen, chronic infections also cause liver inflammation. The family gets their water from a stream that presumably is a habitat for the parasites intermediate snail hosts, with that in mind the girls parents and their neighbours should also be tested for schistosomiasis.
Given the location the most likely species is Schistosoma mansoni.
Praziquantel is the recommended treatment against all forms of schistosomiasis. The Praziquantel Consortium has developed a formulation that is more suitable for younger children [See link below]. According to Parasitic Diseases
Seventh Edition, a short course of steroid medication prior to the use praziquantel can help prevent adverse effects of anthelmintic treatment for acute infection.
Some useful links.
https://journals.plos.org/plosntds/article/file?id=10.1371/journal.pntd.0007617&type=printable
https://www.who.int/news-room/fact-sheets/detail/schistosomiasis
https://www.pediatricpraziquantelconsortium.org/schistosomiasis
https://www.nhs.uk/conditions/schistosomiasis/
Regards
Peter
Mandi writes:
Hello Dickson, Vincent and Daniel from Nashville, Tennessee.
I hope this email finds you all well and settling into the new year. I have a short story to share before I give my case guess that I hope Dickson will enjoy as much as he enjoyed ‘The Tale of the Squirrel and the Botfly’. Each month my 10-year-old son has a book report due at school and the teacher gives them a genre and the students are allowed to pick their own subject from there. This month they have been assigned ‘biography’. I was pitching different subjects to him in the truck on the way to school so help him narrow his search and I asked him if he would want to study someone from science and began to rattle off some of the well-known scientists that would make good subjects for a fourth grade book report. After several suggestions of mine that he rejected, my daughter spoke up and said “What about the parasite guy?” I should note that I have often finished an episode on Twip with my kids in the car and my 7, soon to be 8-year-old daughter is fascinated by twip and often asks me to show her photos of the parasites that have been discussed. I naturally thought any of the Twip hosts would make excellent book report subjects, (information does not solely have to come from a book, but is presented in a report format) but I asked her which one and she said “Dickson-he talks a lot and knows everything.” I chuckled at her summary and asked my son, who seemed to think about it and then decided to keep looking. I hope Dickson isn’t too disappointed not to win the coveted book report position, it’s really an honor just to be nominated.
On to the case. There was not a surplus of diagnostic information in this case so I tried to break it down for analysis. When Daniel first began the presentation I immediately thought of malaria. Then Daniel chipped away at that idea by telling us that the blood smear was negative and again reminded us of this negative smear during Dickson and Vincent’s follow-up questions. The girl was told to return in two days if she felt worse. Being a mom it struck me as odd that she was only instructed to wait two days. Typically when I take my kids to the doctor, the ‘come back if’ time is closer to 4 or 5 days. After reviewing some malaria literature I came to the conclusion that the physicians were using the two day time limit as a diagnostic tool in search of tertian fever. Coupling that with the fact that one negative blood smear does not rule out malaria I believe this girl has malaria caused by plasmodium falciparum. Living in the mountains and not utilizing mosquito nets is a gamble and hopefully swift treatment resolved her illness.
Congratulations on your ‘nomination’ Dickson!
Thank you all again for all that you do, keep on Twippin’.
Sincerely,
Mandi L.
James writes:
Hey, Twips (not TwiRps) So, in summary, 6 y.o. girl with vague systemic complaints, splenomegaly. Fever. Eastern Uganda in mountains.
What would I ask my medical students to do? Create a differential diagnosis!
1. Neoplasm—some kind of lymphoma etc. or Histiocytosis X/eosinophilic granuloma?
2. Sickle cell or other hemoglobinopathy? Bone pain?
3. Autoimmune—young…
4. Metabolic disease? Gaucher etc. but I would not expect fever/constitutional symptoms.
5. Infection
a. Fungus—only Histoplasma duboisii comes to mind, probably wrong part of the continent though
b. Virus—the various TORCH, EBV agents; HIV
c. Bacterial—seen with endocarditis sometimes, typhoid, some others
d. Parasites!
Parasites causing Splenomegaly is actually not that short a list. It IS TWIP after all.
Toxoplasma (the T of TORCH) can do it
Malaria can do it and one negative smear really doesn’t exclude it. Is this the “horse” and not the “zebra” on my list?
Schistosomiasis can do it probably via portal hypertension, 6 seems awfully young for that but it’s on the list
Leishmania (again, so soon after we already did Kala Azar?) clearly can do this
African trypanosomiasis is on the list
Maybe a fluke like Clonorchis or Fasciola? Could be. I think the pathogenesis might be similar to Schistosoma though and she’s a little one.
Echinococcus? Possible.
E. histolytica in liver blocking blood flow? Starting to reach here…
Ascaris going up biliary ducts? Another reach.
So what do we do in a resource poor environment? What would I do if on one of my mission trips to Nicaragua?
Stool O and P x 3, blood smear evaluation (a really OCD one like I did on returning missionaries when practicing pathology.) Not just a quick scan.
Is Ultrasound available? Often is, even out in the sticks, and might help with some of the causes especially if Doppler for blood flow included
Bone marrow aspirate with a direct smear? Possible if you have a good PATHOLOGIST available!
I certainly doubt any molecular tests available, maybe some serologies?
Refer to a bigger city? Expensive in those countries.
Wish I had a single diagnosis to propose but a DDx list seems like the best I can do!
Jim
| James M. Small, MD PhD, FCAPAssociate Professor of Pathology | Achieving New Heights in MedicalEducation |
| Rocky Vista University |
Jim writes:
Greetings Intrepid Aces of the Antimalarial Squadron:
This still looks like a case of Malaria, based on the symptoms presented, despite the negative blood smear. I did consider some other endemic parasites with similar symptoms but none of them seemed quite right. If this is indeed Malaria, then there can be no doubt as to how she got it.
The only delivery system is the infamous and truly awful Anopheles Mosquito. Make no mistake about it, when these little Vampires need a blood meal, they don’t care who they have to take down to get it.
It is early evening at the end of the rainy season and Mosquito Squadron is vectoring-in to deliver its parasitic payload. Alas, at the very same time these mosquitos are decanting parasites, they are picking them up from infected hosts. For some unlucky humans, this process will prove to be fatal.
Fortunately for today’s patient, she is in the right place at the right time and there are effective antimalarial medications to help quell the infection. The combination of drugs to be used will depend on the type of Malaria and the degree of the infection. Unhappily though, this may not be the first time in her life she has had Malaria and it probably won’t be the last.

Hmmm, not everyone seems to agree with my guess this time. Perhaps I missed a more obvious parasite in this case but Dammit Doctors, I’m only a Jim!
TWIP Rules As Always!
Take care,
Jim in Vancouver
Andrew writes:
Kia ora from Pongaroa,
Book not won … yet – is there a signed video version? 😛
My diagnosis for the East Ugandan 6 year old girl feeling poorly with headache, fever and muscle aches.
My guess is that it is probably Visceral Leshmaniasis.
For me there were three parasites that came into question:
Practicing a bit of Bayesian thinking I came to the following probabilities:
Priors:
1. Echinococcus granulosus (hydatids) 10% probability. The parasite can cause cysts in the spleen but the rate of development of the disease and the lack of animal protein in the diet (this is probably not a herding family so dogs would not be in abundance) lead me to give it a low chance .
As an aside, New Zealand has been declared provisionally free from hydatids since 2002 – Yay! Strips of tarmac at the sides of rural roads still exist and this is where working dogs were ‘dosed’ to clear them of the parasite. Sheep dogs are still only allowed to eat cooked offal and livestock carcasses must be quickly buried to stop foraging. Children were very vulnerable to the parasite playing in areas where dogs had defecated.
2. Schistosoma mansoni – 25% probability. The water source for the family is the river so infection is possible via the snail vector through bathing, playing in the water etc. But the lungs are clear indicating the life-cycle dependent migration through the lungs is probably not happening ; so I am keeping this as an alternate diagnosis to…
3. Leishmania donovani. 65% The symptoms all fit and especially the enlarged spleen. The lack of netting is also a factor as the vectors are sand-flies.
Watching Parasitic Diseases Lecture #8: Visceral Leishmaniasis on YouTube gave me the confidence to up the probability of this diagnosis to 80% and to reduce the other two to 5% and 15% respectively.
The video recommends using a highly sensitive and specific rK39 antigen ELISA available in many endemic areas and a bone marrow aspiration, to confirm the diagnosis.
The video indicates that pentavalent antimonials are preferred in Africa but I will leave it to others to be more specific as having misread “parenteral” as “parental” I think have learned enough new words for the day and not being a doctor 🙂
Prevention is sleeping under insecticide-impregnated bed nets and avoiding outdoor activities when the little beasts are biting. We know all about them in Pongaroa – it is amazing how brutal such a tiny insect can be.
The weather here is a summery 25°C and a few clouds are scudding across a milky-blue sky. Which brings me to a pick that might interest some listeners. I use an app called Globe Observer to send ground based pictures of clouds to meteorologists when satellites are passing overhead. It also has a project to map the habitats of mosquitoes which is sponsored by NASA and which will be of use to researchers. The link is https://observer.globe.gov/do-globe-observer/mosquitoes.
And lastly, I have become a proud patron of the Twipiverse of which I get all the podcasts.
nā mihi,
Andrew
Samantha writes:
Dear TWIP hosts,
Greetings from Miami, where it is an extraordinarily pleasant 70F outside. Lots of sun and low humidity. I’ve been a longtime lurker of the podcast and finally have decided to get in on the fun of guessing the cases. When I initially heard this case – falciparum malaria and EBV came to mind. Both have a high prevalence in Sub-Saharan Africa, and can cause fever, headache, and an enlarged spleen. I subsequently ruled out EBV because these manifestations of infection are uncommon in a child this young – usually reserved for adolescents and young adults. Also, seeing how this is TWiP and not TWiV, I decided to move on, of course, not before going down a wormhole of learning about malaria and EBV co-infections and the elevated risk for Burkitt Lymphoma where P. falciparum prevalence is high. I am not impressed by the negative blood smear of this 6 y/o patient. Seeing how the child has pertinent risk factors – it is rainy season, and she sleeps without a bednet, I think that she should be retested. Depending on what the lab has available, LAMP assays other nucleic acid tests may provide a higher sensitivity than a blood smear. According to Parasitic Diseases, 7th Edition, fever, myalgia, headache, and abdominal discomfort are common symptoms of malaria – albeit in children they may present with more non-specific symptoms. Finally, I checked out the epidemiology of malaria in Uganda and found that in children with confirmed malaria, 92% were infected with P. falciparum alone, 0.4% with non-falciparum species, and the rest were falciparum co-infections. Another study found an association between submicroscopic parasitemia and children presenting with fevers in Uganda, indicating a possibility for clinical consequences of submicroscopic infections. For uncomplicated P. falciparum malaria, WHO recommendations are artemisinin-combination therapies.
For completeness, I’d like to discuss that Leishmaniasis also ran through my mind for this child. Eastern Uganda is endemic for visceral leishmaniasis caused by L. donovani, and clinical features in these areas tend to include fever, weight loss, and an enlarged spleen, with the most affected group being males between 5 and 14 years of age. An rK29 rapid antigen test has been found to be highly sensitive and specific for patients in Uganda. Therefore, I would want to run a diagnostic test for this as well.
And there it is! Even if I am not right, I enjoyed the process!
Sam
Katrak, Shereen et al. “Clinical consequences of submicroscopic malaria parasitaemia in Uganda.” Malaria journal vol. 17,1 67. 5 Feb. 2018, doi:10.1186/s12936-018-2221-9
Asua, Victor et al. “Plasmodium Species Infecting Children Presenting with Malaria in Uganda.” The American journal of tropical medicine and hygiene vol. 97,3 (2017): 753-757. doi:10.4269/ajtmh.17-0345
Kevin writes:
Case 179 pediatric tropical splenomegaly.
A 6 y/o girl with an enlarged spleen and an initial negative malaria smear.
Once upon a time (the 1960s), department stores sold formaldehyde preserved frogs. I used just such a leopard frog for my sixth grade (1968) science fair project. I dutifully discussed the frog’s various internal organs but skimmed over the spleen’s function. My interlocutor asked what the spleen did, and countered my cursory reply by stating that “the spleen is a mystery organ.” Here we are in 2020 and though one may live without one, the spleen has many jobs: hematopoeisis, shouldering 25% of the body’s lymphoid tissue, removal of senescent RBCs and is a kind of platelet warehouse.
Forgive this spleen palaver, TWiP has a way of dredging up quasi-relevant memories.
Please allow a few further splenic comments relevant to children. According to the 2019 ‘Up to Date’ entry, 10% of healthy school age children have a palpable spleen tip (this is presumably US children). Many articles contain the maddeningly nebulous statement that hepatosplenomegaly is ‘very common’ in the tropics. I have been unable to come up with a reliable figure of the prevalence of childhood splenomegaly in sub-saharan Africa and would appreciate Dr. Griffith’s estimate of overall childhood splenomegaly in Bududa.
There are many medical and non-medical factors in this case that greatly raise the likelihood of malaria. First, Uganda has one of the highest incidences of malaria in the world with eastern Uganda being described as a “malaria hyper-holoendemic region” (Kotlyar 2014). Additionally, this is rainy season, when transmission peaks. Children are disproportionally affected. She is not using mosquito netting and has the typical malarial symptoms of fever, headache, splenomegaly. The malaria smear was negative, but Stauffer (2009) reports that the standard Giemsa thick blood smear sensitivity for malaria is approximately 85%, certainly enough room for a false negative result. The sensitivity of thick smears is dependent upon level of parasitemia and the experience of the microscopist. With all due respect to WHO directives advising treatment only in proven cases (in low prevalence areas), if it walks like a duck, quacks like a duck, swims like a duck, but the duck-test is negative (by the way, the duck can kill you)….I aver ’tis a duck. Smears of course should be repeated multiple times and supplemented by rapid diagnostic testing if available. It must be remembered that presumptive diagnosis of malaria (i.e. in the absence of a positive smear), even in sub-Saharan Africa, has an accuracy of only around 50%.
Though splenomegaly is a symptom of disease, (the general opinion holds that enlarged organs are bad), there is some speculative evidence that an enlarged spleen volume may be protective against severe malarial disease and might be a marker of ‘semi-immune’ status, though there is conflicting data regarding such hypotheses.
Other parasitic diseases endemic to Uganda that may cause splenomegaly:
1. Visceral leishmaniasis (VL). Though this disease occurs in Uganda, its incidence is much lower than malaria. Okia (2016) lists 408 VL cases in 2003. The WHO Leishmaniasis Country Profile for Uganda lists 140 new cases of VL for 2015. Compare this to the 2018 WHO estimate of 11.6 million annual case of health-facility reported malaria in Uganda. Our patient’s acute and progressive presentation also argues against VL as the diagnosis.
2. Schistosomiasis. This disease is much more common in Uganda than VL. Exum’s 2019 prevalence study in Uganda notes that S mansoni is the predominant species in Uganda with a national prevalence of 25.6% , with peak prevalence of 36% in the 2–4 year old age group. Exum estimates that as many as 10 million Ugandans may be infected with S mansoni. Again, our patient’s acute presentation with rapid worsening is not typical for schistosome infection where a subacute or chronic course would be expected.
3. As always, co-infections must be considered, such as acute malaria infection occurring in a VL or schistosomiasis patient. Bin Mohanna in the 2015 Saudi Medical Journal reports concurrent malaria, leishmaniasis and schistosomiasis in an 8 year old Yemeni boy.
4. A laundry list of non-parasitic splenomegaly associated conditions can be found in the endnotes.
This child should receive the WHO recommended artemisinin-based combination therapy for presumed uncomplicated malaria caused by P. falciparum. Efforts at definitive diagnosis of malaria should continue and supplemented by testing for other agents as the situation dictates. All other supportive measures should be implemented. Use of mosquito nets and other vector avoidance efforts should be emphasized.
Thanks for TWiP induced reveries.
ENDNOTES
SPLENOMEGALY
DEFINITIONS
Up to Date 2019 definition of splenomegaly-
On physical examination, splenomegaly is generally defined as a palpable splenic edge felt >2 cm below the left costal margin.
Shona Wilson (Cambridge Univ researcher-multiple references regarding pediatric splenomegaly): “The spleen was considered moderately enlarged if palpable 3–4 cm below the costal margin in either the mid-clavicular or mid-axillary line or substantially enlarged if palpable >4 cm below the costal margin in either line.”
DIFFERENTIAL DIAGNOSIS
Up to Date 2019 differential diagnosis-
Infectious: mononucleosis (EBV infection), HIV infection, cat scratch disease, infective endocarditis, babesiosis, viral hepatitis
Malignant: ALL, AML, lymphoma, langerhans cell histiocytosis, autoimmune lymphoproliferative syndrome, Castleman’s dz, POEMS syndrome
Hematologic: various hemolytic anemias, portal vein thrombosis
Hepatic dz: biliary atresia, cystic fibrosis, primary sclerosing cholangitis, Wilson dz, alpha-1-antitrypsin def
Inflammatory: SLE, JRA
Immunologic: primary immunodeficiency
Metabolic: Gaucher dz, Niemann-Pick dz, mucopolysaccharidoses, lysosomal storage dz
Space occupying lesions: harmartomas, cysts, hemangiomas
A very interesting look at how affected communities in Uganda perceive and interpret splenomegaly: Social perceptions of splenomegaly in Uganda: from: Community perceptions of paediatric severe anaemia in Uganda. Dhabangi A, et al (2019) PLoS ONE 14(1): e0209476
“Splenomegaly, in addition to being perceived as a sign of severe anaemia, was a dreaded cause of severe anaemia that was perceived as draining blood out of a child even to death, if not treated. These beliefs were found in all three regions, but were strongest in Buganda, followed by Busoga. The local terms used to describe splenomegaly were; ‘ekikubuuko’, ‘akabengo’ and ‘ekibaale’ among the Baganda, Basoga and Banyoro tribes respectively.
In the Buganda region, all six mothers and four out of seven in our first and second FGDs respectively had taken their children to an herbalist for the treatment of splenomegaly, where they cut on the skin over the abdomen:
“It sucks a lot of blood”. “Yes it does; because when you take the child to be cut (by the herbalist), the child does not bleed and the reason you will be given for this, is that it had already sucked the child’s blood”
Most community members believed that an enlarged spleen sucks blood directly from the heart, and that is caused by either malaria or high fever, but one elderly interviewee explained it to be caused by breast milk spilling from the mother’s opposite breast onto the baby’s abdomen during nursing. In addition, community members assigned gender to splenomegaly, depending on the size and its response to local treatment. They believed an enlarged spleen was likely to be ‘female’ if located in the lower part of the abdomen (large) and if it responded quickly to local treatment; while a ‘male one’ is located in the upper part, and poorly responds to treatment: “They say it is brought about by fever; that state when the child is very hot” (R2_FGD1-_Masaka). “I hear the “male enlarged spleen” (‘akasajja’) rests at the upper part of the abdomen while the female one (‘akakazzi’) on the lower part of the abdomen” (R1_FGD1-_Masaka).
MALARIA
Uganda has the third highest number of annual deaths from malaria in Africa and the highest reported malaria transmission intensities in the world.
Malaria in Uganda: challenges to control on the long road to elimination: I. Epidemiology and current control efforts. Yeka A, et al Acta Trop. 2012 Mar; 121(3):184-95.
From the Uganda Ministry of Health: Uganda has the sixth highest number of annual deaths from malaria in Africa, as well as some of the highest reported malaria transmission rates in the world, with approximately 16 million cases reported in 2013 and over 10,500 deaths annually. (healt h.go.ug/programs/national-malaria-control-program)
Diagnostic performance of rapid diagnostic tests versus blood smears for malaria in US clinical practice. Stauffer WM et al ,Clin Infect Dis.2009 Sep 15;49(6):908-13.
sensitivity for the pbs=85%…85% (81 of 95) for the blood smear, NPV=98%. specificity was 100% (no false positives)….he standard Giemsa thick blood smear sensitivity for malaria—approx 85% (per Stauffer 2009 ref)
Malaria diagnosis: a brief review. Tangpukdee N,et al Korean J Parasitol. 2009;47(2):93–102.
“The most important shortcoming of microscopic examination is its relatively low sensitivity, particularly at low parasite levels. ”
Spleen volume and clinical disease manifestations of severe Plasmodium falciparum malaria in African children. Kotlyar, Simon et al.Transactions of the Royal Society of Tropical Medicine and Hygiene vol. 108,5 (2014): 283-9. doi:10.1093/trstmh/tru040
Site of study: Eastern Uganda Mbale region (37 km from Bududa) In areas of stable malaria transmission, childhood spleen rates have been used as an epidemiologic marker of population immunity, exposure and transmission intensity.…the spleen plays a very important role in malaria immunity—studies showing that splenectomy is very deleterious wrt malaria infection…exact mechanism for the role of spleen in malaria immunity is poorly understood but factors postulated: phagocytic and cellular immune mechanisms…..splenic clearance of infected and uninfected RBCs….patients in hi transmission areas have a concomitant high rate of splenomegaly, considered a marker of “semi-immune” status… the study looked at SV (spleen volume) as measured by ultrasound…SMA (severe malarial anemia) defined as HgB<5 gm/dl…CM (cerebral malaria)sx triad of severe malaria= respiratory distress, SMA, CM…..Eastern Uganda is a high malaria transmission area “malaria hyper-holoendemic region”…..study…n=241….the tentative / speculative conclusion in the study is that increased spleen volume (splenic enlargement) may be protective and may be related to enhanced splenic immune function. Other African studies of splenic enlargement in relation to malaria mortality in children have been conflicting……
The hyper-reactive malarial splenomegaly: a systematic review of the literature. Leoni S, ET AL Malar J. 2015;14:185. Published 2015 Apr 29.
The hyper-reactive malarial splenomegaly syndrome (HMS) is a leading cause of massive splenomegaly in malaria-endemic countries. HMS is caused by a chronic antigenic stimulation derived from the malaria parasite. Classic Fakunle’s major criteria for case definition are: persistent gross splenomegaly, elevated anti-malarial antibodies, IgM titre >2 SD above the local mean value and favourable response to long-term malaria prophylaxis. The syndrome is fatal if left untreated.
Microscopic diagnosis of malaria, WHO info sheet: https://www.who.int/malaria/areas/diagnosis/microscopy/en/
WHO guidelines discourage anti-malaria therapy in smear-negative patients, especially in low prevalance areas…to avoid malaria overtreatment,,,WHO currently makes the tentative recommendation that parasite-based diagnosis should be used in all cases of suspected malaria with the possible exception of children in high-prevalence areas and certain other situations.
VISCERAL LEISHMANIASIS
VL/Malaria coinfection (van den Bogaart E, Berkhout MM, Adams ER, et al. Prevalence, features and risk factors for malaria co-infections amongst visceral leishmaniasis patients from Amudat Hospital, Uganda. PLoS Negl Trop Dis. 2012;6(4):e1617. doi:10.1371/journal.pntd.0001617)…Concurrent malaria represents a common condition among young VL patients living in the Pokot region of Kenya and Uganda—in this 6 year, 2400 patient study, 19% had VL/M coinfection. Although these co-morbidities did not result in a poorer prognosis…age < 9 y/o is an important risk factor for VL/M coinfection …with the prevalence among VL patients ranging from 20.8% and 6.4% in Uganda
WHO website https://www.who.int/leishmaniasis/burden/Leishmaniasis_Uganda/en/
Uganda Leishmaniasis Country Profiles ….Uganda is endemic for VL
VL is considered to be endemic in the Karamoja subregion of Amudat district, an area of semi-arid steppe (north-eastern Uganda). The real burden of the disease and its geographical spread remain unknown. Identified risk factors for contracting VL include sitting on termite mounds, treating livestock with insecticides and having a low socioeconomic status. Owning a mosquito bednet is associated with a reduced risk of contracting the disease. CL has been reported for several years. Today, it probably occurs in the foothills of Mount Elgon, but this needs confirmation. The disease is caused by L. aethiopica (Mulago hospital report; Uganda Ministry of Health). A case of CL due to L. donovani, in an HIV coinfected patient living in the Ssese Islands in Lake Victoria, has also been reported.
Leishmaniasis in Uganda: historical account and a review of the literature. Olobo-Okao J, Sagaki P., Pan Afr Med J. 2014;18:16. Published 2014 May 4.
VL article, (based Amudat Hospital, 168 km from Bududa/Mbale–Leishmaniasis—not so common. Still, a problem, but it is dwarfed by the number of malaria cases
SCHISTOSOMIASIS
Schistosoma mansoni among pre-school children in Musozi village, Ukerewe Island, North-Western-Tanzania: prevalence and associated risk factors., Ruganuza DM et al Parasit Vectors. 2015 Jul 16; 8():377.
SCHISTOSOMIASIS VIS A VIS SPLENOMEGALY
Intestinal schistosomiasis of Ijinga Island, north-western Tanzania: prevalence, intensity of infection, hepatosplenic morbidities and their associated factors. Mueller A, et al. , BMC Infect Dis. 2019;19(1):832. Published 2019 Oct 7.Of note to our findings is the high prevalence of S. mansoni infection in pre-school age children (≤6 years) based on both KK technique and POC-CCA test. The age group had also high intensity of S. mansoni infection compared to the older age group. These findings indicate that, S. mansoni infections starts at an early age and with heavy infection intensities, the age group is likely to start developing hepatosplenic disease at early age. In the young age groups, left liver lobe hepatomegaly and splenomegaly have been noted to correlate with heavy intensities of S. mansoni infection. It is worthwhile noting that, in schistosomiasis endemic areas, P. falciparum malaria is also a cause of hepatomegaly and splenomegaly and differential diagnosis especially in young age groups is a requirement…..The relationship between increased age and observation of chronic hepatosplenic morbidities in older ages mainly signifies that, S. mansoni is a chronic infection which requires time for the overt related morbidities such as PPF, hepatomegaly and splenomegaly to develop….Interestingly, our findings noted a degree of hepatosplenic morbidities among children aged < 5 years. The main hepatosplenic morbidities observed in the children was mainly left liver lobe enlargement, splenomegaly and only a small proportion of the children had signs of PPF.
Nalugwa A, Nuwaha F, Tukahebwa EM, Olsen A. Schistosoma mansoni-Associated Morbidity among Preschool-Aged Children along the Shores of Lake Victoria in Uganda. Trop Med Infect Dis. 2017;2(4):58. Published 2017 Nov 5. doi:10.3390/tropicalmed2040058
Using the Kato-Katz technique on one stool sample collected on three consecutive days, 74.9% (686/916) were found infected with S. mansoni; the majority were lightly infected (57.9%), while 22.7% and 19.4% were moderately and heavily infected, respectively… Both liver and spleen were significantly more enlarged in the infected children than in the uninfected children (p < 0.0005), as measured by ultrasonography. Physical palpation of the spleen was more often detected in the uninfected children.
MOST INFECTED CHILDREN IN THE NALUGWA STUDY (80%, N=686) HAD NORMAL SPLEENS. IN ULTRASOUND DATA, UNINFECTED: 25% HAD SPLENOMEGALY (N=230). IN INFECTED: 31% HAD SPLENOMEGALY (N=686)
The prevalence of schistosomiasis in Uganda: A nationally representative population estimate to inform control programs and water and sanitation interventions, Natalie G. Exum , PLOS, August 14, 2019 according to Exum’s map, the Bududa region is not in a high transmission/prevalence part of Uganda this is the first nationally (Uganda) representative study…S mansoni is the predominant species in Uganda national prevalence of 25.6% where the 2–4 year old children had the highest prevalence for schistosomiasis with 36.1% infected. 27.7% of children age 5–10 years old were infected Prior estimates suggested that in Uganda 4 million individuals were infected with schistosomiasis caused by S. mansoni [44] and this study increases that estimate to over 10 million.
OTHER
Leishmaniasis, malaria, and schistosomiasis concurrently in an 8-year-old boy. Bin Mohanna MA. Saudi Med J. 2015;36(4):494–496.
Okia M, Okui P, Lugemwa M, et al. Consolidating tactical planning and implementation frameworks for integrated vector management in Uganda. Malar J. 2016;15:214. Published 2016 Apr 14. doi:10.1186/s12936-016-1269-7 Important table from this article:
A TERMINAL CURIOSITY
In the course of reading about the TWiP 179 case I stumbled upon the mysterious (to me) entity ‘nodding syndrome.’
Nodding syndrome is a pediatric seizure disorder, etiology unknown, that is found in Uganda, South Sudan and Tanzania (sub-Saharan Africa). This illness was first reported in the early 1960s. A 2013 survey in northern Uganda identified 1,600 cases. A “case was defined as reported head nodding (repetitive involuntary drops of the head towards the chest on two or more occasions) in a previously normal person. A probable case was defined as a suspected case with age of onset at 3–18 years and a frequency of nodding of 5–20 nods per minute.” In addition to the neurologic manifestations, affected children can have cognitive impairment, growth stunting and delayed puberty. Various postulated causes for this epileptic syndrome include sorghum consumption, measles, and onchocerciasis infection, though the pathophysiology and etiology still evade understanding.
Prevalence of Nodding Syndrome — Uganda, 2012–2013, Preetha J. Iyengar, MD,July 18, 2014 / 63(28);603-606
An Epidemiologic Investigation of Potential Risk Factors for Nodding Syndrome in Kitgum District, Uganda. Foltz JL et al PLoS One. 2013;8(6):e66419.
Nodding syndrome. Dowell SF, Emerg Infect Dis. 2013;19(9):1374-84.
A comprehensive and readable review of the disease.
Christopher writes:
Good morning Professors,
It is a gloomy 38 F here at stony brook Long Island today. For this months parasite case I believe there are two possibilities that could be infecting the patient. The first possibility is that the patient has a malaria infection and the blood smear gave a false negative result, as many of the symptoms you described are characteristic of malaria. The second possibility is that this girl is suffering from schistosomiasis as this parasite is very common in uganda, and can cause enlarged spleen and fevers. Additionally, because both of these parasites are extremely prevalent in this region, the patient could also be coinfected by these parasites.
In addition to my guess I thought I would share a paper I thought was a good read and that I thought you would all enjoy as well (PDF attached below). The paper is called ” The Meaning of Death: evolution and ecology of apoptosis in protozoan parasites” the paper discusses they evolutionary processes that would lead to a single cell protozoan to undergo programed cell death or “parasite suicide”. I found it to be an interesting read, as I viewed protozoan parasites as “selfish” cells, only interested in making sure they survive and proliferate so the idea that they would have programmed cell death conflicted with this thought.
lastly I thought this reddit post the other day would interest all of you and particularly vincent https://www.reddit.com/r/YouShouldKnow/comments/ea3x5g/ysk_in_the_us_more_people_died_from_the_flu_in/
Summary of what the link says ” in the US more people died from the flu in 2018 than from opiates during the worst year of the opiate epidemic (2017). Go get your flu shot. ” with sources from the CDC supporting it.
Granted the people killed by opiates and by flu are a very different demographic, and that there are many sublethal impacts of opiate addiction, but I thought it was interesting that something that kills as many people as the very serious opiate epidemic is taken casually.
once again thanks for the podcast
Warm regards,
Chris
Leah writes:
Dear TWIPsters,
Hi all! After quite a delay I am finally writing in with another guess. Despite the negative blood smear, given the headache, fever, and splenomegaly I still think we are looking at a case of malaria. According to the CDC (https://www.cdc.gov/malaria/diagnosis_treatment/clinicians1.html), while a negative blood smear makes the diagnosis of malaria unlikely, non-immune individuals (which this young girl in good living conditions could definitely be) can be symptomatic at very low levels of parasitemia, making blood smears challenging. I’m assuming that when the patient came back in on Wednesday, another blood smear was done which may have been positive? Particularly, given the relatively rapid onset of splenomegaly observed, Plasmodium vivax is the most likely culprit. The fever spike after two days also supports P. vivax, as it exhibits tertian fever. If I’m right, I would love to be considered for the hard copy of Parasitic Diseases!
Best wishes,
Leah (PhD candidate in Immunology at UCalgary)
Benjamin writes:
To the TWiP triad,
I believe the Ugandan child is suffering from malaria, most likely caused by Plasmodium falciparum, in spite of her initially negative blood smear. The tertian fever likely rules out P. malariae, although I’m not sure if fever timing is still used frequently for species level malaria diagnosis. The WHO Ugandan country report suggests that P. falciparum is the only malaria parasite of significance in Uganda, however some recent studies have suggested that a reasonable proportion of people in Uganda have been infected by P. vivax. Given the much higher prevalence of P. falciparum, along with the headaches suggestive of neurological involvement, I think this child was indeed infected with P. falciparum but at the time of her initial blood smear her parasitaemia was too low to be detected by microscopy. Blood smear negativity is not uncommon, as symptomatic patients come sometimes present with very low parasitaemia. Treatment in Uganda would be with artemether/lumefantrine.
It is currently a red hot 43oC in Adelaide, South Australia but thankfully there is some rain on the horizon.
Thanks for all the fantastic work.
Regards,
Ben
Ben Liffner
PhD Candidate – Malaria Biology Lab (Wilson Lab)
Research Centre for Infectious Diseases
School of Biological Sciences
The University of Adelaide
WesternU Global Health Track Students: Dana, Steven, and Chris write:
Hello TWiP professors,
We believe the most likely diagnosis to be Visceral Leishmaniasis, also known as Kala-azar, due to her initial presentation of non-specific symptoms and then later high fever and splenomegaly. Additionally, the lack of the mosquito netting could have given the vector, the sand fly, an opportunity to transmit the parasite to her. Treatment would be Sodium Stibogluconate or Amphotericin B.
Given her splenomegaly, differential diagnosis would include toxoplasmosis, visceral larva migrans, and schistosomiasis.
Sincerely,
WesternU Global Health Track Students: Dana, Steven, and Chris
Alida writes:
Hello Professors,
I hope I am not too VL (very late) to Kala and (h)Azar(d) my guess that this may be Kala Azar, VL or visceral leishmaniasis, caused by leishmania donovani.
Sincerely a VL (Very Loyal) fan,
Peter writes:
The case reports a 6 year old girl with headache, fever and muscle aches (myalgia). Malaria smear is negative.
The case location (rural Uganda) and symptoms described resemble a case of Katayama fever or acute schistosomiasis. The enlarged spleen (splenomegaly), fever, feeling poorly and muscle aches are all, according to Parasitic Diseases 7th Edition, Exposure is via contact with cercariae of the Schistosoma parasite in bodies of fresh water. The cercariae penetrate the skin, usually though a hair follicle and acute disease follows 4 to 8 weeks after initial exposure.
According to Sam Loewenberg from the NGO Schistosomiasis Control Initiative (https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(14)60817-5/fulltext) prevalence of schistosomiasis infection in Uganda ranges from 2% to 92% depending on health district and 4 million (out of a total population of 36 million) people are infected with the disease. Edridah Tukahebwa, national coordinator for NTDs in Uganda, links the prevalence of the disease to poor sanitation, as contaminated faeces and urine in turn contaminate water supplies. Once again public health involves much more than doctors and nurses!
Since acute schistosomiasis is an immune hypersensitivity reaction, treatment should be started with corticosteroids. Antihelminthic therapy with praziquantel can then take place some 6 weeks after resolution of acute symptoms, allowing the short term immune reaction time to subside and the worms to mature from their larval stage (against which praziquantel is not effective). Treatment should be repeated 4 to 6 weeks after the first treatment court.
Peter
writing from a sunny Cape Town, where I am about to listen to TWIV 585 (after a visit to the dentist) and can thus far report that I am on one of only two continents that have yet to have a confirmed case of 2019nCoV. I don’t know if that will still be true by the time you read this email.
Cilia writes:
Dear TWiP,
Greetings from Florida! I have just recently stumbled upon your podcast, so I hope I am not too late with this response for case 179. I am a 4th year medical student and have been on the interview trail for internal medicine residency programs over the past few months. Your podcast has kept me entertained and intrigued during my long drives and travels, so thank you all.
After doing some research, I believe the diagnosis may be hyperactive malarial splenomegaly, also known as tropical splenomegaly syndrome. From what I gathered, it results from overstimulation of the immune system in response to repetitive or chronic malarial infections. It would account for her fever, abdominal pain, splenomegaly, and a negative malarial smear. Laboratory testing may show elevated IgM and antimalarial antibody. However, these patients also typically have hepatomegaly and portal hypertension, and on physical exam, no hepatomegaly was noted. Or…perhaps it is malaria, although a negative peripheral smear is not as likely (but possible?).
Thank you all again for this podcast. I am looking forward to the diagnosis and the next case.
Warm regards,
Cilia
UCLAN parasitology club writes:
Dear TWIP Professors,
Hello again from the Parasitology Club at the University of Central Lancashire in the beautiful North West of England.
Our multi-national group of students has been bitten by the parasitology bug and have come up with a list of candidate organisms for this sick six-year-old, and firm favourite amongst them.
On our list of candidates were:
Schistosoma mansoni. It is water borne trematodes (fluke) and symptoms of infection can include, fever, belly pain, cough malaise, headache, rash, body aches, and fibrosis in spleen and liver.
Capillaria hepatica. A nematode parasite with a natural host in wild rodents. Geographically possible in the African region but a rare cause of infection in humans.
However, we believe this could be a case of malaria.
Typical symptoms of malaria are cold, fever (hyperthermia), headache, nausea and vomiting, lack of appetite, muscular pain, convulsion (mostly in children), anaemia followed by splenomegaly at later stages, coma.
Members of our group are from Nigeria, Mozambique and Surinam and have personal experience of malaria and this provides the rest of the group with a fantastic insight into daily life in an endemic region.
Diagnosis can be quickly confirmed by examining thick and thin blood films stained with Romanowsky stain this may also be used in combination with other stains such as Wright-Giemsa and May-Grünwald. A false-negative smear on the blood film is not uncommon so the child may have been asked to return for a repeat smear.
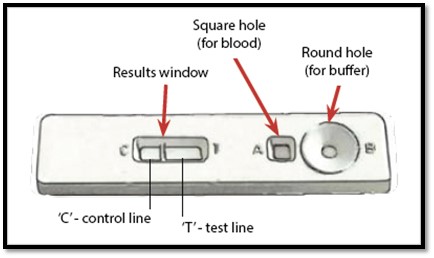
Malaria rapid diagnostic tests are useful in diagnosing malaria by identifying presence of different species of malarial parasites. They are used as an alternative to microscopy due their rapid, handy and inexpensive characteristics. The test normally involves usage of a cassette containing a nitrocellulose strip. Typically, a drop of blood is obtained via a finger prick which is introduced to the sample port along with a buffer solution to carry the reagents along the strip. After a few minutes incubation the results are visible in the form 2 red bands- in the case of positive infection or 1 red band- in the case of a negative infection.
RTDs reduce the pressure on local hospital laboratories in that people can carry out the test in the luxury of their homes. Minimal training is required as the kits come with step by step instructions. In addition, this is advantageous in rural areas where there are minimal resources for quick and proper medical diagnosis.
However, RTDs do not tell which malarial parasite one has been infected with which may lead to inaccurate self-medication and even resistance on the long run.
It is recommended that a positive result on the RTD should be confirmed in a diagnostic laboratory.
Below is an image showing an example of a malarial RTD cassette.
We would be proud to receive a signed copy of PD7 and have our collective fingers crossed that we will be lucky enough to be randomly selected from the TWIPeratti writing in to solve this tricky case.
Thank you again for your wonderfully informative podcasts that stimulate the discussions in our group.
With the warmest regards from the cold North of England.
David, Saleha, Dennis, Abba, Anneke, Katie, Charlotte, Hunynah, Mandy, Jessica and Jo from the University of Central Lancashire Parasitology Club
Dr David Wareing
Lecturer in Medical Microbiology
University of Central Lancashire
ID Team At Karolinska writes:
Dear Professors,
Thanks so much for your interesting and entertaining podcast!
We are a group of Infectious Diseases trainees, nurses and assistant nurses working at Karolinska University Hospital in Stockholm, Sweden. We have used your great case presentation in our weekly teaching session as a means to learn more!
In the latest episode 179 you presented a case of a 6-year old girl in Uganda with a fever and massive splenomegaly.
Our differential diagnoses for massive splenomegaly are chronic schistosomiasis, visceral leishmaniasis, hyper-reactive malarial splenomegaly, and Echinococcus but we also thought about non-parasitic reasons such as lymphoma, ALL/AML or thalassemia major.
Differentiating the non-parasitic diagnoses is likely to be difficult since the necessary blood tests are unlikely to be available in an outpatient clinic in rural Uganda. A low haemoglobin would also be found in many of the differentials we propose. We assume the patient didn’t have any other symptoms such as lymphadenopathy or purpuric rash which may favour a haematological diagnosis. We felt that thalassemia major is unlikely since the patient has survived until 6 year of age. Thalassemia minor would be possible with the potential for thalassemia major having killed other siblings.
Now for the parasitic diagnoses.
We thought that a splenic Echinococcal cyst would be unlikely since this is not the most common place for a cyst and the patient is young. There was no mention of sheep or dogs and her diet was mostly vegetarian. To fit the clinical picture with fever such a cyst would then need to have a secondary bacterial infection.
Chronic schistosomiasis is a valid differential since household water is collected from a nearby stream. The 6-year old girl could be collecting the water for the family and therefore be repeatedly exposed, but we thought that she might be a bit too young for such a massive spleen. Splenomegaly would also require an enlarged and fibrotic liver, something which was not found on examination. Chronic schistosomiasis does also not lead to fever.
Visceral leishmaniasis is also a valid differential which is rather common in this region although we were a bit unsure about Eastern Uganda specifically. Hepatomegaly is usually also seen with this diagnosis as well as weight loss and general lymphadenopathy – which was not mentioned. As visceral leishmaniasis could be quite asymptomatic in the initial phase, this could be the early sign for the disease developing.
Our top differential was hyper-reactive malarial splenomegaly caused by repeated malarial infections. These patients also have negative microscopy for malaria which was true for this girl. Her age fits with having this diagnosis. It was also mentioned that it was currently the rainy season and no bed-nets were available which means higher risk of malarial transmission. To explain the fever and the general malaise she could now have acute malaria with developing symptoms and undetectably low parasite count on Monday. Another option is a concomitant bacterial infection such as Typhoid or non-typhoidal Salmonella infection as these are common with malaria. Thalassemia minor could be consistent with low parasite malarial infections since it is protective from severe malaria.
Our suggestion would be to perform the following tests:
-New smear microscopy for malaria and preferably a rapid test if this is available
-Rapid antigen test for leishmaniasis rK39 if available or smear of splenic aspiration
-Stool examination for ova and parasites to detect eggs of possibly Schistosoma mansoni
-Haemoglobin
For treatment
-If positive malaria test – treat for acute malaria and consider long-term prophylaxis for malaria if no other reason for massive spleen is detected
-Consider treating for acute bacterial infection such as Salmonella/Non-typhoidal Salmonella with ciprofloxacin or ceftriaxone
-Treatment of other diseases depending on test results
If we win the book we will use it in our outpatient day-care clinic where we see a lot of patients with travel history from tropical countries.
Greetings from a snowless wintery Stockholm where it is now 2 degrees Celcius
From the ID trainee team at Karolinska