
Anthony writes:
Permethrin is toxic to cats. Perhaps some mention might be made that cat owners must keep their pets from where permethrin is applied at least until it dries.
Perhaps for those with cats pyrethrin might serve as a substitute? Pyrethrin has very good knockdown, though is lacking in the persistence that permethrin has. Pyrethrin is fine for cats and even can be used directly on them for parasite control. For specific applications, the label directions and the cat’s veterinarian’s advice do need to be followed,
Thank you.
Sophia writes:
Hello doctors
you don’t need to read this out loud but I would like to share a thought with you: how about doing a (special?) episode on co-infection with parasites? like malaria and ebola. A rare coincidence? I would like to know more about how the host responds to co-infection and if infection with a parasite confers an advantage at times (would it? don’t know) or a disadvantage to infection with a virus. I thought this is the perfect show to talk about this since we have a virologist, a parasitologist and an infectious disease doctor. I would appreciate a discussion and stories, not necessarily a paper (sorry I don’t understand most of them). Just a thought
all the best
Benjamin writes:
Dear TWiP team,
A paper was just published in PLoS Pathogens where the authors show that Trypanosoma brucei infection can prevent malaria in a mouse model, I think this would make a really cool paper for you to review on TWiP!
Link to the paper: https://journals.plos.org/plospathogens/article?id=10.1371/journal.ppat.1008145
Regards,
Ben
—
Ben Liffner
PhD Candidate – Malaria Biology Lab (Wilson Lab)
Research Centre for Infectious Diseases
School of Biological Sciences
The University of Adelaide
Case guesses:
Andrew writes:
Hi TWiP trio,
I have not written into the show for a while, but am really hoping to get a book!
Here is my guess for TWiP 177!! If I (with my lack of a medical degree and little travel experience) were in Dr. Griffin’s shoes I think the first thing I would do is treat the patient’s D. fragilis with Metronidazole. The first Ova and Parasite exam showed a commensal parasite, which gives the clue that this patient was exposed to infected feces. That first result should have been followed up with additional stool exams for ova and parasites, but I assume since he was on vacation at an urgent care center, his care was not followed up with properly. The second thing I would do with this patient is order another full Ova and Parasite exam; including a Modified Acid Fast smear for Cyclospora and Cryptosporidium. And I might even add a Microsporidium smear as well. Since this event seems like it was food or drinking water-bourne, I would be suspicious of Cyclospora as well as the D. fragilis.
I am probably totally wrong, but I am not a doctor… I work in the lab looking at these organisms at the other end of clinical care.
Love your show!
Andrew from Boston
Sophia writes:
Hello twipsters
glad to hear about the weather in the last episode.
As for this week’s guess, my answer is: I don’t know. You could say it’s dientamoebiasis although I highly doubt it since there is no eosinophilia detected. There is not enough info in your book to explore this further. I am clueless. What do we do? well, why don’t we wait and see? Personally, if I could lose weight like that I wouldn’t be seeing doctor. I would be thrilled and enjoying it! The only thing I can think of for weight loss is giardiasis but he reports no bloating. Sorry if this was an easy guess. I would still like to win the book though…..
And since this email hasn’t contributed much I will try to make up for it by suggesting a pick : there is a free online course (you have to pay if you want a certificate) on leishmaniasis by LSHTM: https://www.futurelearn.com/courses/visceral-leishmaniasis
the link might have expired by the time you read this but it’s on futurelearn.
All the best from a rainy but still quite warm (20 degrees C) Greece
Andrew writes:
Pongaroa calling,
[Book not won yet – third try – ever hopeful]
The weather here is showers, 14°C and overcast.
My diagnosis is that his gastrointestinal problems were most likely caused by Dientamoeba fragilis contracted while in Hawaii. The Chilomastix mesnili found in the first and second tests is considered practically non-pathogenic so very unlikely to be the cause in a fit 49 year-old. D. fragilis, on the other hand, although often symptom-less is more likely to be the cause of the man’s problem.
The timing of the symptoms lead me to think he contracted D. fragilis in Hawaii and that the Pakistani restaurant is a red herring or red lamb, I assume that the food in the restaurant was eaten by hand and that that would lead one to think of the fecal-oral route of infection. But I think the onset of the symptoms after the meal is too short to be realistic. D. fragilis is often missed in stool samples so that it may have been overlooked in the first. Vincent was right to ask about the Hawaiian salads.
What to do next? What to do next is basically beyond my pay-grade but my wished-for pay is a book and I am still in the running even if I get that wrong – so here goes.
The lost weight. What the heck? Most of us would be happy to lose a few pounds. As he is symptom-free but still has the parasites, I would suggest checking him for pinworms. D fragilis is well named as it the snowflake of parasites and is easily destroyed in stomach acid and does not last long in the environment. There is a hypothesis that helminth eggs could be a way it enters the body -Trojan horse-like, and thus persist as the pinworm eggs are recycled hand to mouth. One could advise the patient to take a double helping of dessert until the desired weight returns (just kidding).
Iodoquinol is generally the drug of choice for the treatment of Dientamoeba. Paromomycin and metronidazole are also effective.
Pongaroa tidbit – we have a small river but it is not great fishing unless you like tuna [rhyme with fun-a] (the Māori name for eels). There is, however, a nearby and fairly deserted beach which attracts surf-casters and boat fishers. So Dixon might like to check it out next time he is in New Zealand.
cheers,
Andrew
Jim writes:
Dear Twipsters:
Thanks for your assurance (in TWIP #177) that there would be no public flogging for a wrong answer.
This case was harder than usual, particularly since Dr. D was not around to pose a hintful question or two. There was some mention of a healthy Hawaiian salad and a delicious lamb dish, but I will not be chewing on those today. No red herring either. Anyways, here it goes.
The patient could have contracted the protozoan D. fragilis in Hawaii or California as it is widespread. The exact mode of transmission for this parasite is not fully understood, but we do know it does not live long in the external environment.
It might have come in through the patient’s mouth via undetected fecal contamination. Perhaps it came in along with its nonpathogenic commensal C. mesnili but this is speculation.
One thing we do know for sure is that D. fragilis can keep some shady company, by hiding inside the eggs of vicious intestinal worms. These worms can hatch and may migrate to other parts of the human body. We also know that the presence of C. mesnili is sometimes associated with unreliable stool sample test results including false positives and negatives.
D. fragilis itself does not cause symptoms in everyone, but it is certainly capable of causing the nausea and diarrhea that this patient had for a week. It follows that he would lose weight during this time due to dehydration, reduced caloric intake and inhibited absorption of nutrients. The fact he has not yet regained all the weight he lost during his illness is not necessarily indicative of an ongoing problem. Since all of his bloodwork is normal and he is not losing weight, it is more a question about whether his current weight is healthy.
In short, two organisms of interest were found in the patient’s stool but there is no direct evidence of another active pathogen. However, because these two particular organisms are sometimes linked to intestinal parasites and because C. mesnili is associated with unreliable test results, multiple deep dives into the stool will be required. We need to find out if D. fragilis is really there and, if so, is it keeping bad company? If microscopic investigation does not yield a definitive result, PCR testing is always an option.
What to do if D. fragilis is the only pathogen left standing at the end of the day. It could be wiped out with a course of Doxycycline but this has to be weighed against all the regular concerns about overusing antibiotics. This really is a question for his doctor.
I would be honoured to win a signed copy of your book.
Here in Vancouver, it is currently 282° Kelvin under partly cloudy skies with rain in the forecast.
TWIP rules as always!
Take care,
Jim
James writes:
I’m writing to you as a new Microbiology professor at Rocky Vista University School of Osteopathic Medicine. (I also get to teach pathology.) After thirty years of private practice in various cancer hospitals doing frozen sections for demanding surgeons, this is a great second career.
So, a 49 year old man, travel to Hawaii and California, Pakistani restaurant (did he have the Red Herring?,) Nausea and Diarrhea. Stool O and P with Chilomastix and D. frag. Feeling better, but 10-15 pounds of weight loss persists. HIV neg.
Differential diagnosis?
1. D. frag COULD do all this. Chilomastix is usually more a “marker organism” for some other infection. But as Bart Simpson once said to his father, “Too easy Homer, too easy.”
2. Giardia could do this. Indeed it HAS done it to me. Gave me some pretty good malabsorption and unmasked my familial lactose intolerance. Once I stopped large chocolate-chocolate milkshakes at Baskin Robbins, a dark day indeed, symptoms lessened a lot and my (then) young children stopped calling me Mr. Stinky. Giardia commonly gets missed on O and P but there is a good antigen test. I wonder if this might be a sneaky Giardia?
3. Hawaii; these symptoms don’t really sound like rat lungworm to me.
4. Clearly he has picked up some protozoa, so somewhere he’s gotten into bad food or water. The sky starts becoming the limit here! Various cestodes, nematodes are on my list. I don’t recall if you mentioned a stool occult blood? Visceral larva migrans from sushi in either state? E. histolytica, a mild case? Stool O and P has a significant false negative rate for many organisms. Cryptosporidium?
5. As an ID dude you’d of course have to consider bacterial infections. Viral seems sort of unlikely with this history, although Hep A is a thought. Did not see liver enzymes. Can’t really think of a fungus among us. I suppose, true-true-unrelated, there are other weight loss things like occult malignancy and autoimmune conditions, any chronic inflammatory state, that would creep onto the bottom of my list as well.
I do believe I’d start with a couple more O and P’s (is three still the magic number?) AND a giardia antigen test before writing this off as D. frag. I’d also throw in a stool occult blood (my ID prof at Mr. Duke’s School of Medicine and Basketball, Ralph Corey, used to say a good doc is not smart, a good doc is complete.) But the GI doc likely did that.
And, I might add, this diagnosis has a lot of commercial potential in a country with massive obesity. Asymptomatic, 10-15 # weight loss? Gold mine!
James M Small MD PhD
Assoc Prof Pathology
Rocky Vista University
Parker, CO
Cecelia writes:
Dear Doctors,
I think the symptoms of Dr. Griffin’s patient were caused by Dientamoeba fragilis.
All the newer literature agrees that the organism can cause weight loss and gastroenteritis symptoms. The presence of Chilomastix mesnilii is probably unrelated to his symptoms since it’s widely accepted to be nonpathogenic.
It’s presence does indicate that the patient probably ate something that was contaminated with feces, since Chilomastix is spread by ingesting contaminated food or water. Since the patient ate salads while on vacation, that could have been the source of the Dientamoeba also.
Since Dientamoeba can be difficult to diagnose in just one specimen, it may have been missed in the first ova and parasite study.
Thanks again for your amazing podcast, and all the other good work you do.
Sincerely,
Cecelia
Saint Petersburg, Fl
Kevin writes:
Polynesian pseudo-polyparasitism?
This case mentions Hawaii, which immediately activated my regrettable Type I mental response and the availability heuristic. Alternatively, has the word Hawaii just exposed my own crude island stereotypes: spam (canned meat, not the electronic variety) , the hula, leis, grass-skirts, angiostrongylus, floral shirts and cornball 50s off-color jokes with the punch-line ‘come-on-I-wanna-lay-ya’.
I usually build up a case analysis with the patient age, location, exposures etc. TWiP 177 somehow discounts all of this. The patient’s age isn’t particularly important. Hawaii- eh? Or is meh the preferred ejaculation; Hawaii is really not a festering disease zone (Nevermind Alicata’s 1964 treatise Parasitic Infections of Man and Animals in Hawaii). The Pakistani restaurant….well, exposures could happen anywhere, let’s not impugn the sanitary conditions of any particular ethnic food service.
But travel, persistent diarrhea and weight loss does call for some concern. I’m a little surprised that the initial medical visit resulted in a stool for O & P, a rather low yield investigation for someone returning from Hawaii. (notwithstanding the 82 cases of angiostrongyliasis from 2007-2017 in Hawaii, though this parasite is not diagnosed via stool.) This first O & P yielded the humble Chilomastix. The dilemma in this case is that our patient has recovered from his episode of diarrhea and weight loss and three months later is re-tested (despite being completely asymptomatic) and his stool is now positive for Chilomastix and Dientamoeba. I realize that he reports a net 5 pound weight loss, however this is insignificant in my estimation, especially when considering the dismal accuracy of reported and measured body weights in the clinical setting. So, how to proceed?
PD7 is gratifyingly unequivocal on the status of the not uncommon flagellate Chylomastix mesnili: it is “considered nonpathogenic by all standard criteria.” Of relevance to us is Garcia’s comment in her 2016 review which states that Dientamoeba may be mistakenly identified as Chylomastix due to a nuclear chromatin similarity. I will leave other Chylomastix digressive material to the vast dumping grounds of my endnotes.
This brings us to Dientamoeba fragilis. Johnson’s 2004 review (referenced in PD7) contains one of the strangest anthropomorphisms of recent times: “Dientamoeba fragilis is struggling to gain acceptance as a legitimate pathogen in many countries.” Johnson’s lament could also be read as a political allegory of current events in Washington. This flagellate organism was described fairly recently: 1918. Transmission is believed to be fecal-oral (what else), has an imperfectly understood life-cycle with a putative cystic form and possible animal reservoirs. The trophozoite has a wide size variation (5-15 microns) and is difficult to positively identify. Multiple authors emphasize the importance of making permanent stained stool preparations as the live organism can only be reliably seen in very fresh fecal smears (hence the name fragilis, named because the organism quickly deteriorates outside of the host gut.) Dientamoeba is not included in current multi-array molecular panels. There seems to be a consensus that this protozoan causes diarrhea (some say up to a third of infected persons may be symptomatic), but there are a few remaining skeptics (see Endnotes). As an example of “adding insult to injury”, it is hypothesized that Dientamoeba may occasionally be a stowaway inside of a pinworm ova, resulting in yet more polyparasitism. 2019 CDC treatment recommendations: iodoquinol, paromomycin, or metronidazole. Tetracycline has also been used.
Our current case recalls TWiP 167, wherein a patient was coincidentally relieved of her chronic constipation after tropical travel and E. hartmanni was a witness to this. TWiP 167 and 177 walk in the shadowlands of medicine, where the question can be asked, who do we treat and why? Our asymptomatic and recovered tourist has some Dientamoeba. Is it now part of his eukaryome and of possible benefit, or does this belly-creeping amoebo-flagellate demand extirpation? Most practitioners would treat and most patients would demand pills.
What would you do?
There may yet be one universal that unites all political persuasions: A well functioning gut is desirable.
Thanks for a solid and regularly moving podcast.
ENDNOTES
Notes on Chilomastix etymology:
mastig—whip, flagellum
chilo–lip, lips
despite fastidious searching I could not find much on the history of the naming of this organism, philologically speaking. I am only speculating that the chilo- part of the word refers to the Greek word for lips.
Mesnili: see ‘A Terminal Curiosity’
In a 2019 surveillance study in Jalisco State Mexico, Galván-Ramirez et al found that 6.7% of children harbored Chilomastix mesnili.
According to the CDC the life-cycle of Dientamoeba fragilis is not completly worked out. Speculation that pigs may be a natural host and human compatible Dientamoeba genotypes have been isolated. However, human to human transmission is believed to be the main route of infection.
Dientamoeba fragilis, One of the Neglected Intestinal Protozoa, Lynne S. Garcia, Journal of Clinical Microbiology Aug 2016, 54 (9) 2243-2250; DOI: 10.1128/JCM.00400-16 OPEN ACCESS
A very comprehensive look at Dientomeba. My random notes below:
…closely related to trichomonads. Very common cause of GI sx, maybe exceeds giardiasis…hard to diagnose using ‘certain’ methods…often overlooked….’neglected’…first described 1918 (Jepps and Dobell) NAMING…was binucleate (hence dientamoeba) and disintegrated quickly outside the body (hence fragilis
a surprising morphology/taxonomy: it is an ‘amoeboflagellate’…related to trichomonas (and Histomonas)
–cyst stage- fecal oral transmissiion
–worm ova transmission possible (similar to Histomonas meleagridis in turkeys-which has a helminth vector). In humans speculation of dientamoeba transmission via ova of Enterobius and/or Ascaris…
–appearance of nuclear chromatin can mimic Chylomastix mesnili, Endolimax nana, or Entamoeba hartmanni.
–5-15 microns. Big size variability…
–chronic sx are common and up to one-third of infected people can have chronic diarrhea
–Lab: must observe organisms in fresh stool samples due to degradation of morphology….also need to prepare a permanent stained smear. Garcia recommends a minimum of three specimens in a 10 day interval
–as of 2016, no commercially available immunoassay. In not included in the BioFire, BD Max enteric and xTAG GI pathogen assay panels
–Current recommendations include iodoquinol, paromomycin, or metronidazole -current CDC recommendations (metronidazole is not FDA approved for this indication
–“D. fragilis was first seen in 1909 by Charles Wenyon after the examination of his own fecal specimen;” Garcia 2016. ? for Annals of Self-Experimentation…. look up… can’t find the original paper. Read the Dobell text for some background info…
Emerging from obscurity: biological, clinical, and diagnostic aspects of Dientamoeba fragilis, Johnson, E. H., et al., Clin Microbiol Rev Jul 2004, 17, 553-70.184
–lack of a suitable animal model
–Perhaps the most striking reason to consider D. fragilis a potential pathogen is that it can be easily treated and that the great majority of patients show significant clinical improvement thereafter
–large size variations: in human specimens: from 3.5 to 12 microns and up t 40 microns in culture
–D.frag is struggling to gain acceptance as a legitimate pathogen in many countries…
–Studies have also demonstrated links between this parasite and urticaria, biliary infections, pruritus, colitis, allergic colitis, irritable bowel syndrome, and diarrhea in people infected with human immunodeficiency virus.
Up To Date
–Chylomastix mesnili—non-pathogenic flagellate
–contributing to the ‘controversy’ that D.frag. may not be pathogenic….specific processing req for dientamoeba means many cases go undiagnosed
–clinical: diarrhea, abd pain/discomfort, anorexia/weight loss, fatigue, nausea
sx may last years (tho association studies with IBS have been negative)
tx (Up To Date 2019)
●Metronidazole (500 to 750 mg three times a day for 10 days)
●Paromomycin (25 to 35 mg/kg per day in three divided doses for 7 days)
●Iodoquinol (650 mg three times a day for 20 days)
●Tetracycline (500 mg [10 mg/kg] orally four times daily for 10 days) or doxycycline (100 mg [2 mg/kg] orally twice daily for 10 days)
Does Dientamoeba fragilis cause diarrhea? A systematic review. Wong, Z.-W., Faulder, K., & Robinson, J. L. (2018). Parasitology Research, 117(4), 971–980.
–The lead: “It remains controversial whether Dientamoeba fragilis is a commensal parasite or a pathogen.”
–their conclusion: There were only two challenge studies involving one person each. In conclusion, the evidence that D. fragilis would cause diarrhea or that treatment would hasten diarrhea resolution is inconclusive.
–a literature review. Authors analyzed association studies, treatment outcome studies, challenge studies. 47 studies were ultimately selected from a raw search that initally included 966 papers.
Enteroparasitism and Risk Factors Associated with Clinical Manifestations in Children and Adults of Jalisco State in Western Mexico., de la Luz Galván-Ramírez M et al, Osong Public Health Res Perspect. 2019 Feb;10(1):39-48. OPEN ACCESS n=104
The prevalence of parasite infections in the study population was 77.9% including: Entamoeba histolytica/E. dispar/E. moshkovskii/E. bangladeshi (37.5%), Giardia intestinalis (11.5%); commensals: Endolimax nana (44.2%), Entamoeba coli (27.9%), Chilomastix mesnili (6.7%) and Iodamoeba bütschlii, (2.9%); emerging intestinal protozoans: Blastocystis spp. (49%), Cryptosporidium spp. (7.7%) and Cyclospora cayetanensis (2.9%); and helminths: Enterobius vermicularis (18.3%) and Ascaris lumbricoides (5.8%). The results also showed that 58.64% of the studied population presented polyparasitism
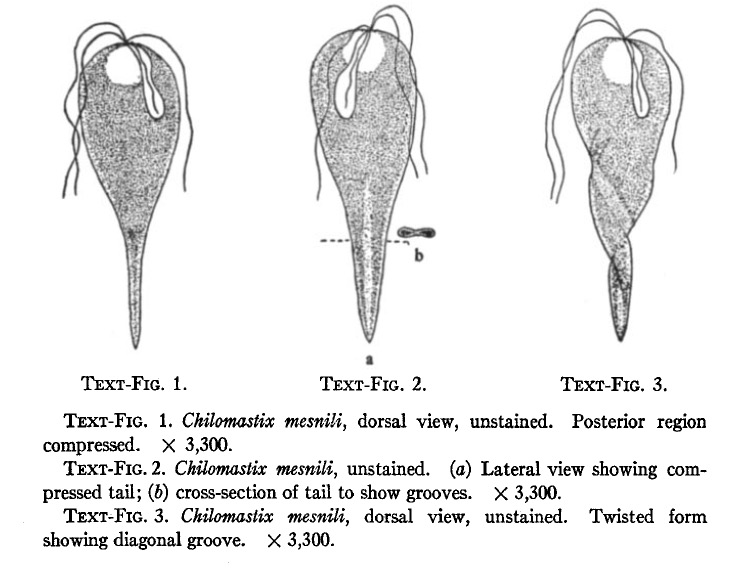
Above illustration from Boeck, W. C. (1921). CHILOMASTIX MESNILI AND A METHOD FOR ITS CULTURE. Journal of Experimental Medicine, 33(2), 147–175. (PUBLIC DOMAIN)
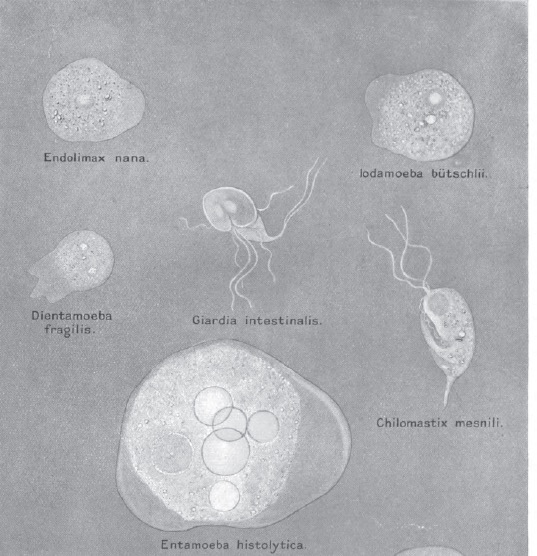
Above illustration from The Intestinal Protozoa of Man, Clifford Dobell and F W O’Connor, London: John Bale Sons & Danielsson, 1921 (PUBLIC DOMAIN)
A Terminal Curiosity
Whether we consider Chilomastix mesnili in our case to be a stalking horse, a straw man, an innocent bystander, a mutualist or commensal, it is clear that its eponymous roots lead directly to the great protozoologist Felix Mesnil, who was born 151 years ago on this December 12.
Mesnil worked at the Institute Pasteur for his entire career and was Director of Colonial Microbiology from 1907-1938. He worked closely with some of the giants of immunology and microbiology: Metchnikoff (discoverer of the macrophage and Nobel prize winner in 1908.), Laveran (discoverer of the causitive agents of malaria and trypanosomiasis and Nobel prize winner 1907.), Roux (developed the first effective anti-diptheria serum.)
In addition to his clinical contributions, Mesnil did basic biological work on protozoans, such as his studies on “the curious protists parasitic on gregarines, the metchnikovellidae.” The metchnikovellidae are “known exclusively as parasites of gregarines inhabiting the intestinal tract of marine annelids.” And you thought your research was arcane.
Mesnil also worked with Maurice Nicolle in the development of treatments for T. gambiense. As an aside, Maurice’s brother was Charles Nicolle, Nobel Prize winner in 1928 for the discovery that lice were the vector of typhus.
Mesnil co-authored the first treatise on trypanosomiasis with Laveran, which was published in 1904 and went through several editions.
In conclusion, I wave a flagellum in honor of this great scientist, on the 151st anniversary of his birth, 12 December 1868.
source: Trans. Roy. Soc. Trop. Med. V.31,Iss.6,20 April 1938 p 691
https://doi.org/10.1016/S0035-9203(38)90162-2
Peter writes:
Greetings to the Knights of the TWIP!
The patient mentioned in TWIP 177 appears to be infected with Dientamoeba fragilis, a flagellum-less flagellate previously thought to not be pathogenic. Stark et al’s 2016 review [1] provides an excellent introduction to this organism. In a somewhat more accessible form, the Government of South Australia provides an introduction to D. fragilis infection [2] that includes in its description of symptoms “abdominal pain, diarrhoea, excess gas, poor appetite, fatigue, nausea, weight loss, vomiting and tiredness” while warning that “[i]t may be that these symptoms are not caused by D. fragilis infection.” This leaves me with a possible answer and some more questions:
1) Why did the D. fragilis not show up on the first O&P?
2) Is the D. fragilis the source for the patient’s symptoms?
3) How was the infection acquired?
4) What is likely to happen to the patient in the future?
5) What treatment is recommended?
On the first, Parasitic Diseases,7th Edition states that while diagnosis using microscopy is possible, “since trophozoites are fragile and not easily detect able on wet mounts, fixed, stained stool sam ples are more sensitive”. After a thorough discussion of staining techniques for detecting D. fragilis, Stark et al note that “D. fragilis trophozoites are shed intermittently, and daily shedding is highly variable” and “even in symptomatic patients, the examination of a single stool specimen could miss a large number of D. fragilisinfections”. It seems then that this parasite is quite easy to miss in an exam, and the negative result from the first O&P could simply be ascribed to chance.
Then, is the D. fragilis the cause of the patient’s symptoms or could there be another cause? Any number of gastroenteric diseases, such as norovirus infection, can cause weight loss, nausea and diarrhea. The presence of D. fragilis, like that of the non-pathogenic Chilomastix mesnili, might be a red herring as D. fragilis infection does not always lead to clear symptoms.
As to how the infection was acquired, the fecal-oral route is most likely, either via direct transmission or via D. fragilis catching a ride on a pinworm.
At the point of examination by Dr Griffin the earlier symptoms seem to have died down. D. fragilis has been known to self-limit thus it is possible that this infection could resolve without intervention. However, to be certain, treatment with trimethoprim-sulfamethoxazole would clear any nagging parasites.
After writing all of the above, I feel that I am flailing at answers without a high degree of certainty. Thus in order to end this email on a high note I enclose three photos taken at the Nigeria Centre for Disease Control’s National Reference Laboratory where they are hard at work performing surveillance as part of the effort to eliminate onchocerciasis. I hope that their survey will deliver good news in the future, but I fear that it might not.
References
1) “Dientamoeba fragilis, the Neglected Trichomonad of the Human Bowel”, Damien Stark, Joel Barratt, Douglas Chan, John T. Ellis, J. Clinical Microbiology https://cmr.asm.org/content/29/3/553
2) “Dientamoeba fragilis infection – including symptoms, treatment and prevention ” – South Australia Health – http://j.mp/37qbvJ1
(being trained in surveillance techniques)

(observing survey results on a Luminex machine)

(the Luminex machine keeps working on backup power even when the lights go out)
Peter
writing from Abuja, Nigeria, where the weather is a warm 30 C.
WesternU Global Health Track Students: Dana, Steven, and Chris write:
Hello TWiP professors,
D. fragilis can cause gastroenteritis-like symptoms as well as weight loss so his symptoms could be entirely due to that and it is associated with chilomastix mesnili. Could be treated with Iodoquinol.
Differential diagnosis for his past symptoms could include Cryptosporidium since it can be spread through contaminated water (which could have been used to wash his salads in Hawaii), and most people who have a healthy immune system will recover without treatment. To determine if this organism is still present, another stool sample could be collected to attempt to identify the acid fast oocysts on microscopy. If present, could treat with nitazoxanide.
For patient reassurance, you could do another O&P. Otherwise, next steps could be patient education on D. fragilis and Chilomastix mesnili and other possible parasitic infections that could have caused his symptoms.
Sincerely,
WesternU Global Health Track Students: Dana, Steven, and Chris
David writes:
Dear TWIP Professors,
Hello from the Parasitology Club at the University of Central Lancashire in the beautiful North West of England.
We would like to add our considered opinion for the very tricky case of the gentleman who visited the Hawaiian Islands and then became sick quite quickly after returning home and having a Pakistani meal with family.
The symptoms are quite typical of infection of the gastro-intestinal tract and the diagnostic algorithm should include bacteria, virus and parasitic causes of infection.
As this is a case for TWIP we have focussed on the parasitic options.
The onset just 24 hours after dining at the Pakistani restaurant is likely too short for an acute infection with an intestinal parasite and I hope the gentleman will continue to consider the meal one the finest that he has eaten and return to the restaurant for more delicious fayre from the East. We believe that the infection would likely have been contracted in one of the Hawaiian islands.
A fantastically detailed treatise on parasites of man and animals on Hawaii by Professor Joseph E Alicata, identifies a long list of organisms to be found on the islands but interestingly there was no mention of Apicomplexan parasites such as Crytosporidium which are a common cause of enteric infection worldwide. Professor Alicata also appears to responsible for the theory that Angiostrongylus cantonensis, the rat lungworm, may be the causative agent of eosinophilic meningoencephalitis of man in the Pacific region and we encountered reports that this parasite has been a cause of recent concern for visitors to the islands. There were 10 cases of this nasty parasitic infection in 2018 and five to date in 2019 and public health officials indicated that the likely cause to be the consumption of an infected intermediate host, a slug or snail, that may have inadvertently wandered into their delicious fresh salads and tarnished their garnish.
The most common parasitic causes of acute diarrhoea in high income countries are Cryptosporidium and Giardia.
The patient does not report bloating or foul smelling, fatty stools more typical of infection with Giardia which has been reported on the Hawaiian islands notably Oahu, and good diagnostic methods are available so we could assume that two negative samples can rule this organism.
Infection with Cryptosporidium became more widely recognised as a human pathogenic parasite when it was associated with HIV infection and was one of the AIDS defining illnesses during the 1980s. AIDS patients suffered intractable diarrhoea and severe weight loss at the hands of the parasite. This patient reports significant weight loss associated with his GI disturbance. The average onset for Cryptosporidium is approximately 2-10 days with an average of 7 days and a duration of 2-3 weeks and is self-resolving in immunocompetent individuals which could fit with the data we have from this patient, however the Hawaiian Public Health Department indicate that this is rare in the region and diagnostic methods in the acute sample should have readily detected the organism.
The laboratory findings of Chilomastix mesnili in both samples from this patient is unremarkable as this organism is considered non-pathogenic.
An excellent review of Dientamoeba fragilis is provided by Stark and colleagues from Sydney, Australia who chart the history of the discovery of the organism and provide evidence for and against the role of this organism as a human pathogen. On balance they indicate that there is likely a pathogenic role for this organism but call for more research into this enigmatic organism. Detection of the organism in faecal samples can be sporadic and this might account for the initial negative sample followed by a positive sample.
With the limited epidemiological details and symptomology being common to a prolonged bout of diarrhoea with concomitant weight loss and the presence of intestinal amoeba indicates a likely exposure the faecal derived organisms, perhaps on the salad vegetables consumed in Hawaii. It is possible that Dientamoeba fragilis could have caused the symptoms and been undetected in the initial sample. So we will take sides with Stark et al and support the hypothesis that D.fragilis has been the aggressor in this sad balad of the bad salad.
We would be proud to receive a signed copy of PD7 and have our collective fingers crossed that we will be lucky enough to be randomly selected from the TWIPeratti writing in to solve this tricky case.
References
Stark D, Barratt J, Chan D, Ellis JT. Dientamoeba fragilis, the Neglected Trichomonad of the Human Bowel. Clin Microbiol Rev. 2016;29(3):553–580. doi:10.1128/CMR.00076-15
PARASITIC INFECTIONS OF MAN AND ANIMALS IN HAWAII by Joseph E Alicata
https://core.ac.uk/download/pdf/5104850.pdf
Dr David Wareing
Lecturer in Medical Microbiology
University of Central Lancashire
Preston.
Amanda writes:
Hello Dickson, Vincent and Daniel from Tennessee!
I am so excited to finally be writing after lurking for what may be considered an inappropriately long amount of time. I stumbled on to a Twip podcast while on a small road trip to deliver a Bald Eagle to the American Eagle Foundation in Pigeon Forge, Tennessee. I had ran out of episodes to catch up on with my regular podcasts and decided to google science podcasts and my search was rewarded. So thank you for keeping me company as I drove my patient to the sanctuary. Eagles are very sensitive to sounds and I had to rely on my earbuds to deliver the parasitic parfait of Twip. I should note that I am a wildlife rehabilitator and a surgical receiving technician at a veterinary specialty hospital, otherwise riding around with an eagle in my truck sounds a bit odd. Due to my work with wildlife I have had a wonderful opportunity to see some parasites that most people do not get to see. One of my favorite episodes to date focused largely on bot flies. I was probably a little too excited about it, but I have had the opportunity to extract them from various species including white-tail fawns, raccoons and eastern cottontails. Perhaps the most interesting extraction was from the testicle of an easter grey squirrel…upon his release back to his home territory he was greeted by several other squirrels and many clicks and squeaks and tail displays ensued. I can only translate this exchange as “It’s all fun and games until you get a botfly in your nuts.”
This email is getting rather lengthy so I will venture my guess for twip 177.
I stared at the show notes for this episode for a bit, thinking I was missing something, and I still think that I am but the testicle bot fly is a cool story and a stab at a diagnosis is a good cover for it. Daniel said that chilomastix and d. fragilis came up in the stool analysis. I’m pretty sure this man had traveler’s diarrhea. Chilomastix is non-pathogenic and d. fragilis is a major contributor for intestinal troubles such as those experienced by our patient. Azithromycin should clear him up if my guess is correct. This case is also a good example of how men and women approach the same situation very differently. This man loses 15 pounds and gains 5 back and wants to know why he didn’t gain the other 10…..a woman would not care and probably not mention it aloud lest the whole 15 pounds hear her and come running back. I kid of course, but only slightly. I look forward to hearing the conclusion of the case as I feel it seems more obvious than most of the cases and if I am wrong I would like to hear about what clue I missed to help in the future.
Thank you for all your time, effort and dedication!
Appreciatively,
Mandi L.
Rufus writes:
Hi all:
I love TWIM, TWIV and TWIP. I contribute annually.
But I have to admit I’m not a fan of all the flying you all seem to do. As far as the podcasts go, I don’t think I’d notice if Vincent did the interviews of groups in Australia from Boston or Melbourne, but if we could make academic travel more of an exception than the rule, the world would be better off.
Here’s a change.org petition which addresses this issue and suggests some reporting metrics:
https://www.change.org/search?q=Academic%20flying
As to metrics, how about this one: perhaps for travel to far exotic clinics your institutions could record the ratio of [hours worked in a remote clinic] to [miles traveled to reach the clinic]. 0.02 seems a reasonable minimum benchmark. My neighbor did a clinical trip to Tibet last year and her talk made it seem pretty much a vacation – 2 weeks of sightseeing, 5 days in the clinic (which she highly enjoyed).
I work in industry and have been making similar suggestions about our corporate travel. For example, we shouldn’t be able to keep air miles. Companies should use them. If they want to reward folks for the hassle and family separation due to corporate travel, that reward shouldn’t be in the form of more travel. Rewards should be carbon neutral.
Best regards,
Rufus
Portland, OR